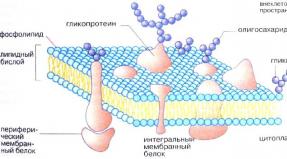
Treatment of functional dyspepsia. Dyspepsia Functional dyspepsia of the stomach
Thanks
The site provides reference information for informational purposes only. Diagnosis and treatment of diseases should be carried out under the supervision of a specialist. All drugs have contraindications. Expert advice is required!
What is dyspepsia?
 Dyspepsia is a collective term denoting various digestive disorders, mainly of a functional nature. It is not an independent symptom, but rather a syndrome.
Dyspepsia is a collective term denoting various digestive disorders, mainly of a functional nature. It is not an independent symptom, but rather a syndrome. The dyspepsia syndrome includes a complex of symptoms that reflect disorders gastrointestinal tract (from the Greek dys - violation, peptein - digest). The duration of symptoms in dyspepsia syndrome is 3 months or more. The clinical picture includes pain or discomfort in the epigastric region, bloating, and sometimes stool disorders. Most often, these symptoms are associated with eating, but can also be caused by emotional overload.
In recent decades, scientists have noted a close relationship between stress and dyspepsia syndrome. Apparently, it is no coincidence that the term "dyspepsia" was widely used in medicine in the Middle Ages and denoted a disease caused by nervous disorders along with hypochondria and hysteria.
Causes of dyspepsia
 There is a wide variety of causes that can cause dyspepsia. Very often, several causes and / or risk factors are simultaneously involved in the development of this syndrome. The modern concept of the causes of dyspepsia has been actively developed in recent years. Today scientists are possible causes, contributing to the development of dyspepsia, consider a number of factors, namely hypersecretion of hydrochloric acid, dietary errors, bad habits, long-term medication, Helicobacter Pylori infection, neuropsychiatric and other factors.
There is a wide variety of causes that can cause dyspepsia. Very often, several causes and / or risk factors are simultaneously involved in the development of this syndrome. The modern concept of the causes of dyspepsia has been actively developed in recent years. Today scientists are possible causes, contributing to the development of dyspepsia, consider a number of factors, namely hypersecretion of hydrochloric acid, dietary errors, bad habits, long-term medication, Helicobacter Pylori infection, neuropsychiatric and other factors. The causes of dyspepsia are:
- stress;
- genetic predisposition;
- biliary pathology ( bile) systems;
- pathology of the gastrointestinal tract ( gastrointestinal tract).
Helicobacter pylori and other bacteria in the development of dyspepsia
An important role in the development of dyspepsia is played by the microbial factor, namely Helicobacter Pylori. Many researchers confirm the etiological role of this microorganism in the formation of dyspepsia syndrome. They are based on data from the clinical picture of dyspepsia in patients with Helicobacter Pylori. They also believe that the severity of the syndrome is related to the degree of contamination of the gastric mucosa. This theory is supported by the fact that after antibiotic therapy (against Helicobacter) manifestations of dyspepsia are significantly reduced.Confirmation that the state nervous system plays an important role in the development of dyspepsia, is the fact that stressful situations often provoke a deterioration in the condition of patients with this disease.
Genetic predisposition to dyspepsia
In recent years, research has been actively conducted to identify the genetic predisposition to dyspepsia. As a result of these studies, a gene was identified that is associated with the work of the digestive organs. Disruption of its expression may explain this pathology.Pathology of the biliary system
In the hepatobiliary system of the body, the formation of bile occurs continuously. The gallbladder serves as a reservoir for it. In it, bile accumulates until the moment it enters duodenum. From the gallbladder during digestion, bile enters the intestine, where it participates in the process of digestion. Bile demulsifies ( breaks down into small particles) fats, facilitating their absorption. Thus, the biliary system takes an important part in digestion, and therefore the slightest dysfunction can provoke the development of dyspepsia.The most common functional disorders of the biliary system, namely various dyskinesias ( motor disorders). The prevalence of these disorders ranges from 12.5 to 58.2 percent. In persons over 60 years of age, functional disorders of the biliary system are observed in 25 to 30 percent of cases. It is important to note that dyskinesia predominantly affects women. Functional disorders of the biliary system include functional disorder of the gallbladder, functional disorder of the sphincter of Oddi, and functional pancreatic disorder.
The flow of bile into the digestive tract is provided by the accumulative function of the gallbladder and its rhythmic contractions. With each meal, the gallbladder contracts two to three times. If this does not happen, then bile begins to be secreted in insufficient quantities. Insufficient participation of bile in the process of digestion provokes symptoms such as heaviness in the epigastrium, nausea and others. This is explained by the fact that the lack of bile leads to the fact that food fats are not absorbed by the body, which explains the symptoms of dyspepsia.
Pathology of the gastrointestinal tract in dyspepsia
Various diseases of the gastrointestinal tract can also be the cause of dyspeptic syndrome. It can be gastritis, peptic ulcer or pancreatitis. In this case, we are not talking about functional, but about organic dyspepsia.The most common disease that manifests itself as symptoms of dyspepsia is gastritis. Chronic gastritis is a disease that affects more than 40 to 50 percent of the adult population. According to various sources, the frequency of this disease is approximately 50 percent of all diseases of the digestive system and 85 percent of all diseases of the stomach.
Despite this prevalence, chronic gastritis does not have a specific picture and is often asymptomatic. Clinical manifestations are extremely variable and nonspecific. Some patients may show "flaccid stomach" symptoms, while others may show "irritable stomach" symptoms. However, most often, patients have symptoms of intestinal dyspepsia, namely flatulence, rumbling and transfusion in the abdomen, diarrhea, constipation, and unstable stools. This symptomatology can be supplemented by astheno-neurotic syndrome ( weakness, fatigue).
The second most common is gastric ulcer. This is chronic illness occurring with periods of exacerbation and remission. The main morphological feature of this disease is the presence of a defect ( ulcers) in the wall of the stomach. Leading symptom peptic ulcer is pain. This takes into account its periodicity, rhythm and seasonality. In contrast to functional dyspepsia, in this case there is a clear relationship between food intake and the appearance of pain. According to the time of appearance, they can be divided into early ones, ( 30 minutes after eating), late ( two hours after eating) and "hungry", appearing 7 hours after the last meal. In addition to pain symptoms, the clinical picture is manifested by various dyspeptic phenomena - heartburn, nausea, belching. All these and other symptoms indicate a violation of the evacuation of food from the stomach. Appetite, as a rule, does not decrease, and sometimes even increases.
Types of dyspepsia
 Before proceeding to the existing types of dyspepsia, it is necessary to divide dyspepsia into organic and functional. Organic dyspepsia is one that is caused by certain diseases. For example, it can be peptic ulcer, reflux disease, malignant tumors, cholelithiasis and chronic pancreatitis. Based on this, organic dyspepsia is divided into gastric, intestinal and other types of dyspepsia. If, with a thorough examination, no diseases can be identified, then we are talking about functional ( non-ulcer) dyspepsia.
Before proceeding to the existing types of dyspepsia, it is necessary to divide dyspepsia into organic and functional. Organic dyspepsia is one that is caused by certain diseases. For example, it can be peptic ulcer, reflux disease, malignant tumors, cholelithiasis and chronic pancreatitis. Based on this, organic dyspepsia is divided into gastric, intestinal and other types of dyspepsia. If, with a thorough examination, no diseases can be identified, then we are talking about functional ( non-ulcer) dyspepsia. Depending on the causes, there are several types of dyspepsia. As a rule, the same symptoms are characteristic of all of them. The difference between them is the reason for their development and the peculiarity of pathogenesis ( occurrence).
Types of dyspepsia are:
- gastric dyspepsia;
- fermentative dyspepsia;
- putrefactive dyspepsia;
- intestinal dyspepsia;
- neurotic dyspepsia.
gastric dyspepsia
In most cases, the presence of symptoms of dyspepsia is associated with pathology of the stomach and duodenum ( upper intestine). At the heart of gastric dyspepsia are such frequent illnesses like gastritis, reflux, peptic ulcer. This pathology is widespread among the population, and it accounts for about one third of all clinical cases. Gastric dyspepsia is characterized by polymorphic ( diverse) clinical picture, but the severity of its symptoms does not correlate ( not related) with the severity of mucosal damage.The syndrome of gastric dyspepsia is manifested by pain in the epigastric region, which is not associated with impaired bowel function. The duration of symptoms is at least 12 weeks.
Many experts in the development of gastric dyspepsia assign the main role to the microbial factor, namely Helicobacter Pylori. Proof of this are studies that have shown that the elimination of this factor leads to a decrease or complete disappearance of the symptoms of gastric dyspepsia. Yes, in the background antibacterial treatment there is a positive dynamics of morphological changes ( these changes are visible on fibrogastroduodenoscopy). Other scientists and clinicians deny the etiological role of this microbe in the development of gastric dyspepsia syndrome. Anyway, application antibacterial drugs in order to remove this microbe from the body is not a mandatory item in the treatment of gastric dyspepsia.
Fermentative dyspepsia
Fermentative dyspepsia is a type of dyspepsia, which is based on excessive gas formationcaused by fermentation. Fermentation is the process of splitting products in anoxic conditions. The result of fermentation are intermediate metabolic products and gases. The reason for fermentation is the intake of a large amount of carbohydrates into the body. Instead of carbohydrates, insufficiently fermented foods, such as kvass, beer, can act.Normally, carbohydrates are utilized ( are absorbed) in the small intestine. However, when there are a lot of carbohydrates, they do not have time to be metabolized and begin to “roam”. The result of this is excessive gas formation. Gases begin to accumulate in the intestinal loops, causing bloating, rumbling and colicky pains. After passing gas or taking antiflatulents ( espumizan) the above symptoms subside.
Symptoms of fermentative dyspepsia include:
- bloating;
- colicky pains;
- stool 2 to 4 times a day.
Putrid dyspepsia
Putrid dyspepsia is a type of dyspepsia, which is based on intense processes of decay. The processes of decay are caused by protein foods, as well as some inflammatory processes in the intestines. Protein food in this case becomes a substrate for pyogenic flora, which triggers putrefactive mechanisms. Clinical manifestations putrid dyspepsia are symptoms such as bloating, frequent diarrhea ( stool up to 10 - 14 times a day). The feces at the same time become dark in color and acquire a fetid odor.In the diagnosis of putrefactive dyspepsia great importance acquires microscopic examination of feces. Microscopy reveals many undigested muscle fibers.
Intestinal dyspepsia
Intestinal dyspepsia is a symptom complex that combines digestive disorders and enteral syndrome. Clinically, it is expressed in flatulence, impaired stool ( polyfeces), pain syndrome. With intestinal dyspepsia, the stool becomes very frequent, from 5 times a day or more. The pains are bursting in nature and are localized mainly in the mesogastrium.At the same time, enteral syndrome is manifested by metabolic disorders, in particular, a violation of protein and lipid metabolism. Mineral metabolism disorders are also present. Since vitamins are absorbed in the intestine, hypovitaminosis is detected when it dysfunctions ( hypovitaminosis A, E, D). This can lead to dystrophic changes in other organs.
biliary dyspepsia
The basis of biliary dyspepsia is the pathology of the biliary tract. Most often, these are functional disorders ( i.e. dyskinesia), in the development of which stress is of great importance. Since the nervous system plays a leading role in the regulation of the contractile function of the gallbladder and bile ducts, then any stressful situation can lead to the development of gallbladder dyskinesia. The pathogenesis of biliary dyspepsia can be very variable, but always comes down to dysregulation of biliary tract motility. This means that under the influence of trigger factors ( stress, violation of the alimentary regime) there is a change in the motility of the biliary tract, which can be expressed either in its strengthening or in its weakening. Both lead to the development of symptoms of dyspepsia.When the motility of the biliary tract changes, the volume and composition of the ejected bile changes. Since bile plays an important role in the process of digestion, any changes in its composition lead to dyspeptic manifestations. In addition to psychogenic factors, the development of functional biliary pathology is influenced by hormonal imbalance. Thus, an imbalance between the production of cholecystokinin and secretin provokes an inhibitory effect on the contractile function of the gallbladder.
The cause of biliary dyspepsia can also be diseases such as hepatitis, cholangitis, cholecystitis. In this case, the development of dyspepsia is associated with inflammatory changes in the biliary tract.
Symptoms of biliary dyspepsia
The clinical picture of biliary dyspepsia is due to the degree of motor dysfunction of the gallbladder. Pain symptoms dominate. In this case, pain can be localized both in the epigastrium and in the right upper quadrant of the abdomen. The duration of pain varies from 20 to 30 minutes or more. As with functional dyspepsia, the pain in this case does not regress after defecation or after taking antacids. In biliary dyspepsia, the pain syndrome is associated with nausea or vomiting.
Dyspepsia syndrome in psychiatry or neurotic depression
Dyspepsia syndrome occurs not only in the practice of a gastroenterologist, but also in a psychiatrist. Somatic symptoms, stubbornly pursuing the patient for 2 years, without the presence of any organic lesions, are part of the structure of various psychosomatic disorders. Dyspepsia syndrome can mask diseases such as depression, anxiety and panic disorder. Most often, dyspepsia is observed with depression. So, there is a type of depression, which is called masked. He is not characterized by such classical complaints as depression, low mood, and a labile emotional background. Instead, somatic, that is, bodily complaints, come to the fore. Most often, these are complaints from the cardiovascular or gastrointestinal system. The first category includes symptoms such as heart pain, shortness of breath, tingling in the chest. Gastrointestinal symptoms include epigastric pain, nausea, and discomfort after eating. Thus, dyspepsia syndrome can remain the main symptom of depression for a long time.Symptoms of neurotic dyspepsia are:
- nausea;
- belching;
- heartburn;
- pain in the epigastric region;
- difficulty swallowing;
- discomfort in the stomach, intestines;
- intestinal disorders;
To date, more than 250 bodily complaints have been described that occur in depression. In general, the variety of complaints can be so great that it makes diagnosis difficult. A diagnosis requires at least four bodily symptoms in men and six in women. The difficulty of diagnosis lies in the fact that patients do not complain of depressed mood or any other emotional states. However, with prolonged observation, irritability, fatigue, poor sleep, internal tension, anxiety, and depressed mood can be detected.
functional dyspepsia
 According to the new classification, functional dyspepsia is a complex of symptoms that occurs in adults and children older than one year. Functional dyspepsia includes pain, nausea, a feeling of fullness in the stomach, as well as bloating and regurgitation. Also, for patients with functional dyspepsia, intolerance to fatty foods is characteristic. The duration of symptoms must be at least 3 months in the last six months. The term "functional" means that during the examination it is not possible to identify an organic disease.
According to the new classification, functional dyspepsia is a complex of symptoms that occurs in adults and children older than one year. Functional dyspepsia includes pain, nausea, a feeling of fullness in the stomach, as well as bloating and regurgitation. Also, for patients with functional dyspepsia, intolerance to fatty foods is characteristic. The duration of symptoms must be at least 3 months in the last six months. The term "functional" means that during the examination it is not possible to identify an organic disease. The prevalence of functional dyspepsia, like many other functional digestive disorders, is very high throughout the world. So, among Europeans, every fifth suffers from functional dyspepsia, and every third in the USA. At the same time, the percentage of women suffering from dyspepsia significantly exceeds the percentage of men with a similar disease. Functional dyspepsia is noted among all age groups, however, as they grow older, its frequency of occurrence increases.
Prevalence of functional dyspepsia among different age groups
Reasons for the development of functional dyspepsia
pathogenesis ( set of mechanisms) the development of functional dyspepsia has not been studied enough to date. It is believed that functional dyspepsia is a disease based on impaired regulation of the motility of the digestive tract, namely the stomach and duodenum. Proper motor disturbances in this case include a decrease in the accommodation of the stomach to the food entering it and a delay in gastric emptying due to reduced motility. Thus, there is a disorder in the coordination of those links that regulate the contractility of the gastrointestinal tract, which leads to the development of dyskinesia.Visceral hypersensitivity also plays a key role ( hypersensitivity internal organs ). It is she who causes disorders in the adaptation of the stomach to incoming food and difficult evacuation from it. Disturbed accommodation of the stomach to incoming food is observed in more than 40 percent of patients. The consequence of this are symptoms such as rapid satiety, a feeling of fullness in the stomach and pain after eating. Gastric secretion in functional dyspepsia, as a rule, is not disturbed.
Also, most patients with functional dyspepsia have duodenal dysfunction. It is expressed in increased sensitivity to acid coming from the stomach. The consequence of this is a slowdown in the motility of the organ and a delay in the evacuation of the contents from it. As noted above, patients with functional dyspepsia are characterized by intolerance to fatty foods. This intolerance is due to hypersensitivity to fats.
Recent studies suggest that a substance called ghrelin plays an important role in the development of functional dyspepsia. Ghrelin is a peptide synthesized by the endocrine cells of the stomach. With functional dyspepsia, there is a violation of the secretion of this peptide, which normally regulates the digestive organs. Active secretion of ghrelin in healthy individuals occurs on an empty stomach, which stimulates the motor activity of the stomach and gastric secretion. Studies have shown that the level of ghrelin in the blood on an empty stomach in patients with functional dyspepsia is much lower than in healthy people. This causes the development of symptoms such as a feeling of rapid satiety and fullness in the stomach. It was also found that in patients suffering from dyspepsia, the level of ghrelin in the blood plasma after meals does not change, while in healthy individuals it decreases.
Symptoms of functional dyspepsia
Functional dyspepsia is characterized by repeated pain attacks in the upper abdomen. Unlike irritable bowel syndrome, in functional dyspepsia, pain and a feeling of fullness do not go away after a bowel movement. Also, the symptoms are not related to changes in stool frequency. Basic distinctive feature This pathology is the absence of signs of inflammation or other structural changes.According to the Rome diagnostic criteria, there are several variants of functional dyspepsia.
Options for functional dyspepsia are as follows:
- Ulcer-like functional dyspepsia characterized by epigastric pain on an empty stomach such "hungry" pains are very characteristic of stomach ulcers, from which the name). Pain syndrome passes after eating and antacids.
- Dyskinetic functional dyspepsia accompanied by discomfort in the upper abdomen. Discomfort worsens after eating.
- Nonspecific functional dyspepsia. Complaints present in this variant of dyspepsia do not refer to any particular type of dyspepsia.
It should be noted that this classification is typical only for adults. Since it is difficult to obtain an accurate description of complaints in children, in pediatric practice functional dyspepsia is not classified.
In patients with functional dyspepsia, the quality of life is significantly reduced. It is associated with the above symptoms ( pain and nausea), as well as the fact that there is a need to limit yourself to certain foods and drinks. Diet and constant pain provoke social problems. Despite the fact that dyspepsia is functional in nature, the degree of decrease in the quality of life in such patients is comparable to organic pathology.
An important feature of functional dyspepsia is its consistency. AT varying degrees all the digestive organs are affected. So, more than 33 percent of patients also have symptoms of gastroesophageal reflux, while the frequency of signs of irritable bowel syndrome is almost 50 percent.
Dyspepsia in children
Dyspepsia is typical not only for adults, but also for children. Their course of dyspepsia, as a rule, is characterized by a favorable prognosis. Manifestations of dyspepsia in children are very variable and extremely unstable.Doctors assign the main role in the development of dyspepsia syndrome in children to Helicobacter Pylori and the phenomenon of dyskinesia. This is confirmed by studies proving an increase in the prevalence of infection with this microorganism in children with dyspepsia syndrome. While in children who do not suffer from dyspepsia, the infection rate is much lower. Also in children there is a positive trend in the use of antibacterial agents aimed at the destruction of the microbe.
An important role in the development of dyspepsia in children is played by motor disorders of the stomach. It has been established that only 30 percent of children have a normal evacuation function of the stomach. In children who do not suffer from dyspepsia, this percentage reaches 60 - 70 percent. Also, in these children, an expansion of the antrum of the stomach on an empty stomach and after eating is often detected. The degree of expansion correlates ( interconnected) with the severity of dyspeptic syndrome. In addition to the bacterial factor and dyskinesia, cerebral pathology is considered as an etiological factor ( birth trauma), age features functioning of the neuroendocrine system.
For children and adolescents with dyspepsia, appetite disorders such as bulimia and anorexia are characteristic.
Diagnosis of dyspepsia in children
Research plays an important role in the diagnosis of dyspepsia syndrome in children.
gastroduodenal pathology. For this purpose, fibrogastroduodenoscopy is performed ( FGDS), direct and indirect detection of Helicobacter Pylori. Also in the diagnosis, the history of the disease plays a significant role, namely the presence of such symptoms as hungry night pains, discomfort in the upper abdomen, belching of acidic contents, heartburn.
Diagnosis of dyspepsia
 Dyspepsia syndrome is one of the most frequent manifestations gastrointestinal pathology. More than 5 percent of initial applications for medical assistance caused by dyspepsia. In gastroenterology, dyspepsia syndrome is one of the most common complaints. As already noted, there are two types of dyspepsia - organic and functional ( non-ulcerative). The first is characterized by the presence of pathology, for example, ulcers, gastritis, duodenitis. Functional is characterized by the absence of any gastrointestinal lesions.
Dyspepsia syndrome is one of the most frequent manifestations gastrointestinal pathology. More than 5 percent of initial applications for medical assistance caused by dyspepsia. In gastroenterology, dyspepsia syndrome is one of the most common complaints. As already noted, there are two types of dyspepsia - organic and functional ( non-ulcerative). The first is characterized by the presence of pathology, for example, ulcers, gastritis, duodenitis. Functional is characterized by the absence of any gastrointestinal lesions. Diagnostic criteria for dyspepsia are as follows:
- Feeling pain or discomfort localized in the epigastric region. Pain is subjectively assessed by the patient as an unpleasant sensation or a feeling of “tissue damage”.
- Feeling of fullness and stagnation of food in the stomach. These sensations may or may not be food related.
- fast saturation is perceived by the patient as a feeling of fullness in the stomach immediately after the start of a meal. This symptom does not depend on the amount of food taken.
- Bloating perceived as a feeling of fullness in the epigastric region.
- Nausea.
Dyspepsia according to the ICD
According to international classification diseases of the tenth revision ( ICD-10) dyspepsia is encoded with the code K10. However, this type of dyspepsia excludes neurotic or nervous dyspepsia. These two varieties of dyspeptic syndrome are related to somatoform dysfunction of the autonomic nervous system and therefore are not included in the section of gastrointestinal pathology.The diagnosis of dyspepsia is based on the patient's persistent symptoms of dyspepsia for at least 12 weeks per year. With functional dyspepsia, organic diseases should not be detected, and irritable bowel syndrome should also be excluded.
Differential diagnosis of dyspepsia
Symptoms of dyspepsia are found in patients with irritable bowel syndrome, enteritis, stomach cancer. This must be taken into account when carrying out differential diagnosis. To exclude the above diseases, instrumental and laboratory tests are carried out. These include general and biochemical blood tests, coprogram and fecal analysis for occult blood, ultrasound procedure ( ultrasound), endoscopic and X-ray examination ( x-ray).
Instrumental and laboratory studies for dyspepsia
Method | What is being done for? |
Fibrogastroduodenoscopy(FGDS) | Excludes ulcer, gastritis, pancreatitis or other organic pathology of the gastrointestinal tract. |
Ultrasound procedure(ultrasound) | Detects or excludes cholelithiasis, chronic pancreatitis. The method is informative for biliary dyspepsia. |
Scintigraphy with technetium isotopes | Determines the rate of gastric emptying. |
Electrogastrography | Registers the electrical activity of the stomach and the contraction of its walls. At healthy person the frequency of contractions of the stomach is about 3 waves per minute. |
Gastroduodenal manometry |
Functional dyspepsia (FD) is one of the most common causes referral to a gastroenterologist. This condition mainly occurs in young and young people and is a syndrome popularly known as "indigestion" of the stomach. It can occur for a number of reasons and is always manifested by a combination of unpleasant symptoms that cause discomfort, deterioration of well-being and a violation of the quality of human life. Only a specialist can answer the question of what functional dyspepsia is; it is possible to eliminate this syndrome after finding out the cause of its appearance.
The term "dyspepsia" in Greek means a disorder in the digestion of food. It was introduced into clinical practice as early as the century before last to refer to various digestive disorders in infants and initially assumed their functional nature, which was not based on morphological changes in organs.
In subsequent years, dyspepsia began to be called all the symptoms (with the exception of abdominal pain) that appear as a result of a violation of the normal functioning of the gastrointestinal tract (gastrointestinal tract).
 Usually this is not one, but a whole set of signs united by a common etiology, localization and origin, therefore the term “functional dyspepsia syndrome” is more accurate.
Usually this is not one, but a whole set of signs united by a common etiology, localization and origin, therefore the term “functional dyspepsia syndrome” is more accurate.
The gastrointestinal tract is quite easily exposed to various kinds of influences, which lead to the disruption of the work of its various departments, which is manifested by temporary digestive disorders and the occurrence of dyspeptic symptoms.
In some pathological situations that are not related to the digestive system (diseases of the heart, kidneys), similar symptoms may also appear.
It is possible to distinguish gastric dyspepsia from the pathology of other organs by the following characteristics:
- there is always a temporary connection with the functional activity of the stomach or intestines (eating, defecation);
- there is a dependence on the quality of products, volume, type and method of cooking;
- digestive disorders are pronounced and come to the fore (heartburn, nausea, retching).
When a patient contacts a gastroenterologist with complaints of dyspeptic disorders, the doctor always faces the question of what it is - a simple indigestion or a sign of a serious illness.
 There are two main types of dyspepsia:
There are two main types of dyspepsia:
- Organic - is established after an examination and the detection of serious morphological changes in the digestive tract (gastritis, stomach or duodenal ulcer, gastroduodenitis, oncology, cholecystitis, pancreatitis). It is more common in the middle and older age category of patients as secondary disorder digestion against the background of an existing disease. It is eliminated as the treatment of the underlying pathology is carried out, which is an indicator of the effectiveness of therapy.
- Functional - does not have a clear etiology, it is based on a violation of the motor-evacuation function of the stomach or intestines. FD is said to be when a person has been disturbed by indigestion for at least 12 weeks during a calendar year, and the examination did not reveal any organic pathology. In other words, no inflammatory, dystrophic or metabolic lesions mucosa of the gastrointestinal tract. This is the most common group of dyspepsia - 60% of all visits to a gastroenterologist, occurs mainly in childhood and young age.
Causes and mechanisms
The etiology and pathogenesis of functional dyspepsia continue to be studied, there is still no consensus on the mechanisms of development of this condition. However, the predisposing factors contributing to the appearance of this syndrome are precisely known.

The functional form of dyspepsia can occur under the following circumstances aggravating digestion:
- non-compliance with the diet, long breaks between meals, followed by overeating;
- food on the go and dry food, insufficient mechanical processing of food, swallowing poorly chewed pieces;
- the presence in the diet of foods that promote gas formation (mushrooms, nuts, white cabbage, legumes);
- inadequate food quality, abundance of fats, insufficient content of vegetable fiber;
- passion for carbonated drinks (kvass, beer), including those with caffeine;
- alcohol and tobacco abuse;
- psycho-emotional trauma, stress - contribute to spasms in the bile ducts and vessels of the digestive system;
- long-term use of certain drugs (NSAIDs - non-steroidal anti-inflammatory drugs, corticosteroids);
- physical labor or exercise immediately after a meal - blood flows to working muscles, and not to the stomach;
- infection with the bacterium Helicobacter - you can become infected both at home and during medical procedures.
 In practical medicine, there are two main groups of functional disorders. Dyspepsia associated with an insufficient amount or activity of enzymes involved in the digestion of food.
In practical medicine, there are two main groups of functional disorders. Dyspepsia associated with an insufficient amount or activity of enzymes involved in the digestion of food.
These situations are typical for children early age, in adults occur with functional failure of different parts of the gastrointestinal tract:
- pancreatogenic disorder - with insufficient production or poor quality of enzymes produced by the pancreas;
- gastrogenous variant of dyspepsia - with impaired secretion of the gastric glands;
- cholecystogenic disorder - when the process of bile secretion is disrupted;
- hepatogenic form of dyspepsia - with insufficient functional activity of hepatocytes (hepatic parenchyma cells) due to inflammation or other reasons;
- enterogenic - develops due to reduced production of intestinal juice;
- mixed form.
Nutritional dyspepsia is the most common group of functional disorders that occur due to a violation of proper eating behavior. Usually disappear after the normalization of the diet and correction of the diet.
This group is divided into several subgroups depending on the nature of the diet:

- fermentation - occurs due to the excess content of carbohydrates in the diet, as well as the constant use of bread kvass and beer, which do not have time to be digested sufficiently in conditions of increased physical activity small intestine, which causes increased gas formation, loose stools with foam and a sour smell;
- putrefactive dyspepsia - develops with a predominance of proteins in the diet, with secretory insufficiency of gastric juice, with the colonization of the upper gastrointestinal tract by microbial flora from the large intestine, with this type of functional dyspepsia, the symptoms of intoxication are pronounced - headache, weakness, nausea, as well as diarrhea of a putrid odor and dark color;
- fatty - happens from an excess of refractory fats of animal origin, which must be digested for a long time, which causes a feeling of excess filling and heaviness in the stomach, bloating and pain in the abdomen, while the stool is plentiful with a greasy sheen.
Separately, neurotic dyspepsia is noted, which is a consequence of traumatic situations, depressive states, often occurs in emotionally labile people with an unstable psyche.
Clinical manifestations
 Functional digestive disorders can occur in an acute form or exist for a long time in the form of a chronic disruption of the gastrointestinal tract. Simple acute form quite often happens in children transferred to artificial feeding, for example, due to violations of the diet, overfeeding, or from infectious causes. Food toxic dyspepsia is a severe digestive disorder, for the development of which infectious agents. They can come from outside with poor-quality food or be inside the body in the presence of bacterial inflammatory processes (otitis media, sinusitis, pneumonia).
Functional digestive disorders can occur in an acute form or exist for a long time in the form of a chronic disruption of the gastrointestinal tract. Simple acute form quite often happens in children transferred to artificial feeding, for example, due to violations of the diet, overfeeding, or from infectious causes. Food toxic dyspepsia is a severe digestive disorder, for the development of which infectious agents. They can come from outside with poor-quality food or be inside the body in the presence of bacterial inflammatory processes (otitis media, sinusitis, pneumonia).
Depending on the localization of motor disorders in the upper or lower gastrointestinal tract, all dyspepsia is divided into gastric and intestinal forms.
Combined species are possible with damage to the digestive tract throughout.
 Functional gastric dyspepsia is also called "lazy stomach" and the symptoms are as follows:
Functional gastric dyspepsia is also called "lazy stomach" and the symptoms are as follows:
- feeling of heaviness, fullness and stretching in the upper abdomen;
- frequent belching of ordinary air or food eaten;
- halitosis (bad breath);
- appetite disorders;
- nausea, urge to vomit;
- bitter taste in the mouth;
- hypersalivation (increased salivation and salivation).
For intestinal dyspepsia, the following symptoms are characteristic:
- bloating, swelling of the abdomen, flatulence;
- rumbling, transfusion and other sounds in intestinal loops;
- stool disorders - constipation, diarrhea or their alternation.

Depending on the prevalence of individual symptoms in the clinic, the following types of functional dyspepsia are distinguished:
- ulcerative variant - pain in the upper abdomen (epigastric region) predominates, occurring periodically at night during sleep or on an empty stomach (2 hours after a meal);
- dyskinetic variant of dyspepsia - mainly concerned about the feeling of heaviness and overdistension in the stomach, the rapid onset of saturation from small amounts of food, nausea, bloating of the upper floor of the abdominal cavity;
- nonspecific dyspepsia - mixed signs are characteristic.
What to do
 With the infrequent occurrence of individual symptoms of dyspepsia and a clear reason for their appearance, you should not panic.
With the infrequent occurrence of individual symptoms of dyspepsia and a clear reason for their appearance, you should not panic.
In this case, you should pay attention to the following recommendations:
- normalize the diet, avoid overeating and snacking on the go;
- monitor the quality of food;
- organize a meal in a calm leisurely atmosphere;
- avoid participating in stressful situations;
- do not take any strong drugs without consulting a doctor;
- not to engage exercise within an hour or two after the end of the meal.
In the absence of organic changes in the gastrointestinal mucosa, these measures will be sufficient to stop dyspepsia. Otherwise, it is necessary to examine and clarify the diagnosis.
 The following situations should be the reason for contacting a doctor:
The following situations should be the reason for contacting a doctor:
- dyspeptic disorders first appeared after the age of 40;
- the symptoms are constantly disturbing for a week with a clear tendency to worsen;
- symptoms appeared unexpectedly and have a pronounced degree of intensity - nausea, repeated vomiting, heartburn, abdominal pain (this may be a sign of pathology of the digestive tract or heart, it is necessary to differentiate urgently).
Functional non-ulcer dyspepsia syndrome is the most common problem in young and young patients and has a favorable prognosis. With a long-term existence of chronic indigestion, it is necessary to undergo an examination by a gastroenterologist to clarify the diagnosis in order to avoid late detection of a serious pathology.
The term "dyspepsia" is relatively often used by doctors in their practical work when examining patients, but it is often interpreted in different ways, although this term literally means indigestion. Nevertheless, in practice, when it comes to patients with dyspepsia, symptoms such as pain and discomfort that occur in the abdomen during a meal or at various times after it, flatulence, and stool disturbance are most often taken into account.
Etiopathogenetic aspects of dyspepsia. Dyspepsia as a symptom of many diseases of the gastrointestinal tract is relatively common in both functional and organic diseases. Various causes can lead to the symptoms commonly included in dyspepsia syndrome. Functional dyspepsia in gastroenterological practice is detected in 20-50% of cases, while in most patients it is combined with chronic gastritis. The risk of functional dyspepsia is associated not only with a violation of the diet, but also with the intake of non-steroidal anti-inflammatory drugs by patients, as well as with such seemingly “non-traditional” factors as low educational level, rental housing, lack of central heating, joint sleep (in siblings), being married. In some patients, the appearance of symptoms of dyspepsia may be associated with smoking and even with psychological disorders.
For functional dyspepsia, the absence of any noticeable gastrointestinal (including the esophagus) lesions is considered characteristic. This implies only the presence or absence of gastritis and excludes not only relatively small focal lesions (ulcers, erosions), but also diffuse lesions, in some cases relatively large in extent, such as reflux esophagitis, sarcoma, gastric lymphomatosis, etc.
Currently, more and more often "chronic gastritis" is considered as a morphological concept, including a complex of inflammatory and degenerative changes in the gastric mucosa. Various clinical symptoms that appear in some patients, previously usually associated with inflammatory changes in the gastric mucosa and considered characteristic of chronic gastritis (in the absence of organic changes in the stomach), are now considered as functional manifestations that are not due to those morphological changes that make up the essence of the concept " gastritis".
The pathogenesis of functional dyspepsia syndrome, both in general and most of its symptoms, is still unclear. However, it has been noted that dyspeptic disorders in functional dyspepsia, including those combined with chronic gastritis, are possible in patients with weakened motility of the antrum of the stomach, leading to a slowdown in the evacuation of the contents of the stomach into the duodenum, which is probably based on a violation of antrumduodenal coordination , with an intermittent nature of gastric dysrhythmias (rhythm disturbances). Only the pathogenesis of the symptom of rapid gastric satiety associated with a slowdown in gastric emptying seems to be clear enough.
However, in some patients with normal motor function of the stomach, symptoms of functional dyspepsia are also possible (including patients with gastroesophageal reflux disease), which is most likely due to visceral hypersensitivity of the stomach, mainly to distension. Hypersensitivity of the stomach to distension may be associated with impaired receptor perception of normal stimuli, including muscle peristaltic contractions, as well as stretching of the walls of the stomach with food. In some patients, dyspeptic disorders are also possible with increased secretion of hydrochloric acid (due to an increase in the duration of contact of the acidic contents of the stomach with its mucous membrane).
Perhaps there is a serial connection between clinical symptoms functional dyspepsia, in particular the appearance of discomfort after eating (especially after eating foods and drinks that irritate the gastric mucosa), and weakening the relaxation of the stomach. Indeed, many reports indicate an increase in the incidence of clinical symptoms characteristic of functional dyspepsia after the ingestion of certain foods by patients, but there are almost no reports indicating that the use of any food leads to a decrease or disappearance of these symptoms.
Symptoms of functional dyspepsia. Most of the clinical symptoms noted in organic dyspepsia are also found in functional dyspepsia. Among the symptoms of functional dyspepsia, the following can be distinguished: a feeling of heaviness, fullness and fullness of the stomach, premature (rapid) saturation, "bloating" of the abdomen after eating; the appearance of nonspecific pain, burning in the epigastric region, heartburn, belching, regurgitation, nausea, vomiting, regurgitation, salivation, anorexia. The frequency of development of certain symptoms of functional dyspepsia, the time of occurrence, intensity and duration, according to our observations, may be different. The complex of all symptoms that are considered characteristic of functional dyspepsia, during a period of significant deterioration in the condition of patients, occurs only in a small part of patients; in particular, according to our observations, among patients hospitalized in a hospital - in 7.7% of cases (in 13 out of 168 patients).
Most patients with functional dyspepsia, including those combined with chronic gastritis, are relatively rarely examined and treated not only in hospitals, but also in outpatient settings. Only a few patients, when their condition worsens, go to the doctor, insisting on hospitalization in a hospital to clarify the diagnosis and treatment.
When examining patients with chronic gastritis with functional dyspepsia, hospitalized at the Central Research Institute of Gastroenterology, pain in the epigastric region was noted in 95.5% of cases, nausea - in 13.4% of cases; a feeling of heaviness in the epigastric region - in 91.1% and a feeling of early satiety that occurs during or immediately after eating - in 87.5% of cases; belching - in 67.9%, "bloating" of the abdomen - in 77.7% of cases.
Apparently, differences in the contingent of examined patients with functional dyspepsia affect the frequency of development of certain symptoms of this syndrome, presented in the literature by various researchers. So, according to other data, in patients with functional dyspepsia, pain in the upper abdomen was established only in 36% of cases: only 60% of these patients complained of pain that occurs after eating, 80% of patients were disturbed by night pains (at the same time abdominal pain that prevented patients from sleeping - in 89.3% of cases). Patients noted a feeling of early satiety in 85.7% of cases, burning (heartburn), mainly in the epigastric region, in 88.4% of cases, and nausea in 92.9% of cases.
It is well known that periodically occurring heartburn (burning) is possible in patients with normal contact of hydrochloric acid with the mucous membrane of the esophagus and / or stomach (43%); in such patients, the normal pressure of the lower esophageal sphincter is 10 mm Hg. Art. and more. Approximately 30% of people who constantly take antacids to eliminate heartburn (burning) have an increased visceral sensitivity of the esophagus to mechanical or chemical stimuli (with normal data from esophagoscopy and daily pH-metry). In contrast to organic dyspepsia, such a symptom characteristic of dyspepsia as a feeling of rapid satiety after eating is noted only in patients with functional dyspepsia. In addition, excessive belching and vomiting in the morning are more likely to disturb patients with functional dyspepsia.
Unfortunately, the description of the various symptoms that are considered characteristic of dyspepsia in general, including functional dyspepsia, as well as the interpretation of these symptoms by different patients, introduce some confusion when comparing the data obtained and presented by various researchers. In particular, pain in the abdomen (and even behind the sternum) can be "interpreted" by patients as a burning sensation, spasm and an indefinite sensation, heartburn - as a burning sensation not only behind the sternum, but also in the epigastric region, regurgitation - as the "appearance of acid" in the oral cavity.
Diagnosis of functional dyspepsia. It is known that the diagnosis of functional dyspepsia is established on the basis of the study and analysis of symptoms, anamnesis of the disease, the results of a physical examination of patients, as well as data from laboratory and instrumental examination, in essence, by eliminating organic diseases, in which there were symptoms of dyspepsia, i.e., exclusion of organic dyspepsia.
It has been repeatedly proposed, when making a diagnosis of functional dyspepsia, to take into account certain timing of the onset of symptoms that are considered characteristic of this syndrome, the frequency of their occurrence, duration (for a certain time, including within one year), but this approach is unlikely to the examination of patients will find wide application. The intensity, frequency and time of onset of symptoms of dyspepsia may vary. At the same time, a significant part of patients get so used to the symptoms of dyspepsia that they often do not pay attention to them (and do not perceive them as a manifestation of any disease for a long time). Sometimes certain drugs are taken (without consulting doctors) in order to eliminate discomfort various types. And finally, most often the patient cannot remember exactly the time of occurrence of many dyspeptic disorders, the frequency of their occurrence (even the symptoms that are intense in severity). Therefore, as a rule, the beginning of the development of functional dyspepsia, and often its course, the doctor can trace only approximately from the words of patients.
Differential diagnosis. In the differential diagnosis of symptoms of dyspepsia, the following should be taken into account: in 40% of cases, symptoms of dyspepsia occur in patients with benign gastric and duodenal ulcers various etiologies, with gastroesophageal reflux disease and gastric cancer. In 50% of patients, the cause of the appearance of clinical symptoms of dyspepsia remains unclear, so they are often mistakenly considered as manifestations of functional dyspepsia. That is why in the differential diagnosis of organic and functional dyspepsia, along with the clarification of the symptoms and anamnesis of the disease and the analysis of the data obtained, the results of such objective methods as endoscopic and radiographic examination, ultrasonography are essential (in doubtful cases); in some cases, when examining patients, computed tomography is also indicated. The use of these methods allows you to identify or exclude the presence of other diseases (including the cause of organic dyspepsia).
The authors of some publications, reporting on functional dyspepsia, do not agree on the allocation of one or another of their symptom complex. We note the two most common classifications of functional dyspepsia. According to one of them, ulcer-like, dyskinetic, associated with dysmotility, and non-specific variants are distinguished; while reflux-like dyspepsia is considered as part of the symptomatic complex of gastroesophageal reflux disease. However, according to another classification, the following variants of functional dyspepsia are distinguished: a variant associated with impaired motility, ulcer-like dyspepsia, reflux-like dyspepsia and non-specific dyspepsia.
Our own observations suggest that the division of functional dyspepsia into different types can only be regarded as highly arbitrary. Only some patients have the opportunity to identify one or another set of symptoms that can be more or less accurately associated with one of the variants of functional dyspepsia, especially if one adheres to the definition of functional dyspepsia proposed by the compilers of the Rome criteria for functional diseases of the gastrointestinal tract. When making a diagnosis of functional dyspepsia, it is proposed to consider the following criteria:
- the presence of persistent or intermittent dyspepsia occurring within 12 weeks per year, not necessarily consecutively over the last 12 months;
- absence of organic diseases of the gastrointestinal tract with similar symptoms;
- preservation of symptoms of dyspepsia, not associated with irritable bowel syndrome, in which the condition of patients improves after defecation.
As practice shows, in the majority of patients with functional dyspepsia during the period of treatment of patients with a doctor, it is often quite difficult to determine the variant of dyspepsia to select the most optimal treatment option. To a certain extent, this is due to the fact that during the period of contacting a doctor, the patient may not be disturbed by all the symptoms that, according to the anamnesis of the disease, have persisted for 12 weeks or more during the last year. Only if there are many symptoms, it is possible to more or less accurately determine the variant of functional dyspepsia. Therefore, according to our observations, when choosing drug treatment it is advisable to take into account, first of all, the main symptoms of dyspepsia, causing the patient the greatest concern.
Therapy of functional dyspepsia. The main goal of treating patients with functional dyspepsia is to improve the objective and subjective state, including the elimination of pain and dyspeptic disorders.
The success of the treatment of patients with functional dyspepsia is largely determined by the following factors:
- perseverance and friendliness of the doctor in relation to patients;
- the attitude of the patient to his health;
- discipline of patients in relation to food intake, medicines, compliance with general preventive recommendations;
- correction of lifestyle, improvement of its quality.
It is known that in the treatment of patients with functional dyspepsia, including those combined with chronic gastritis, in our country the following medications (or their combinations) are most often used (depending on the condition of the patients): prokinetics (dommperidone, metoclopramide), antisecretory drugs (proton pump inhibitors, H 2 receptor antagonists), non-absorbable antacids (bismuth tripotassium dicitrate (denol)), enzyme preparations (festal, micrasim, panzinorm, penzital, etc.). Sometimes in patients with chronic gastritis associated with Helicobacter pylori (HP), and combined with functional dyspepsia, antihelicobacter therapy is carried out, during which bismuth tripotassium dicitrate (de-nol) or proton pump inhibitors are more often used as basic drugs.
The presence of a large number of drug therapy options offered for the treatment of patients with functional dyspepsia, to a certain extent, indicates the dissatisfaction of doctors with the results of treating patients with functional dyspepsia. This is probably due not only to insufficient knowledge of the pathogenesis of most symptoms of dyspepsia, but also to the pathogenesis of the functional dyspepsia syndrome in general, as well as to the difficulties that often arise when differentiating variants of functional dyspepsia according to a complex of certain symptoms. This is due to the fact that the interpretation of many symptoms of dyspepsia by patients in different populations, including ethnic groups, varies significantly.
As prokinetics in the treatment of patients with functional dyspepsia, domperidone (Motilium, Motonium) or metoclopramide (Cerucal) is usually used. These drugs enhance the peristalsis of the esophagus and stomach, and also ensure the normalization of gastroduodenal coordination and gastric emptying, an increase in the tone of the lower esophageal sphincter. The use of these drugs is indicated in patients with functional dyspepsia who have symptoms such as delayed gastric emptying (feeling of early satiety that occurs during meals or immediately after eating a small amount of food), as well as symptoms associated with increased sensitivity of the stomach to distension (feeling of heaviness , distension and / or overflow of the stomach that occurs during or immediately after a meal); in the presence of heartburn (burning). The usual dose of prokinetics is 10 mg 3 times a day 20-30 minutes before meals. In severe cases, the dosage of prokinetics can be increased to 10 mg 4 times a day (the last time at night), until the intensity of pronounced manifestations of dyspepsia decreases, then continue treatment of patients with drugs at the usual dosage.
When using domperidone (motilium, motonium), there is a lower likelihood of side effects compared to metoclopramide. Therefore, if necessary, domperidone can be used in the treatment of patients for a longer time, but not less than 3 weeks.
Treatment of patients with domperidone eliminates the feeling of premature satiety in 84% of cases, bursting in the epigastric region - in 78%, discomfort after eating - in 82% and nausea - in 85% of cases. Unfortunately, the terms of treatment of patients (this applies to all prokinetics) quite often exceed 2-5 weeks.
To eliminate severe pain and / or heartburn (burning) in the epigastric region in patients with functional dyspepsia, it is quite enough to use proton pump inhibitors at a standard dosage once a day for the first 7-10 days (lansoprazole, pantoprazole, rabeprazole, esomeprazole, respectively, 30 , 40, 20 and 40 mg), after which patients can be transferred to treatment with H2 receptor antagonists (ranitidine or famotidine, respectively, 150 mg and 20 mg 2 times a day). It is known that omeprazole (Losek) at a dose of 20 mg can, on average, reduce the daily level of hydrochloric acid secretion in the stomach by 80%, ranitidine at a dose of 300 mg per day by an average of 60%, which to a certain extent determines the effectiveness of these drugs. The above course of treatment is advisable to carry out in persons with functional dyspepsia with an ulcer-like variant or in the presence of reflux-like dyspepsia in patients.
However, is it always necessary to significantly inhibit acid formation in the stomach for successful treatment patients with functional dyspepsia, including those combined with chronic gastritis? This question involuntarily arises before doctors and researchers due to the fact that hydrochloric acid also plays a certain protective role in the human body; in addition, an excessive decrease in the secretion of hydrochloric acid increases the likelihood of an increase in the microflora in the stomach. It is also known that proton pump inhibitors and H 2 receptor antagonists are more effective in hydrochloric acid hypersecretion. Therefore, in the treatment of patients with functional dyspepsia in a non-specific variant, as well as some patients with impaired motility of the upper gastrointestinal tract, it is advisable to use bismuth tripotassium dicitrate, which has a cytoprotective effect on the gastric mucosa. He is prescribed 120 mg 4 times a day; if necessary, to eliminate pain as an on-demand therapy, it is advisable to additionally take one of the H 2 receptor antagonists 1-2 times a day at a therapeutic dosage until pain and burning sensation in the epigastric region are eliminated.
And yet, the main thing in the treatment of patients is treatment with one or more drugs, the mechanism of action of which makes it possible to eliminate the symptoms of functional dyspepsia, which cause the greatest concern to patients. In particular, in the presence of frequently recurring symptoms of dyspepsia, usually combined under the single term "discomfort", in patients with functional dyspepsia, enzyme preparations (pancreatin, microzym, festal, penzital, panzinorm, etc.) should be used, even with normal exocrine pancreatic function, in necessary cases, combining their use with H 2 receptor antagonists or with prokinetics, with bismuth tripotassium dicitrate. A certain improvement in the processes of digestion and the normalization of the motor function of the gastrointestinal tract help to eliminate the symptoms of functional dyspepsia associated with increased visceral sensitivity of the stomach to stretching, mechanical and chemical stimulation, as well as impaired motor skills.
The duration of treatment of patients is determined by their general condition, which largely depends on the attitude to one's health and the implementation of the recommendations of doctors.
It is equally important to teach patients to observe the regime of work and rest, to avoid taking certain products that are poorly tolerated by them; advise them to seek medical attention in a timely manner if necessary.
Functional dyspepsia and NR. When considering whether there is an association between functional dyspepsia and HP three aspects must be taken into account.
- Syndrome of functional dyspepsia is possible in patients and in the absence of chronic gastritis.
- Functional dyspepsia syndrome can be combined with chronic gastritis, not associated with HP.
- Functional dyspepsia syndrome, may be combined with chronic gastritis associated with HP. Only in this case does it make sense to consider the question of the appropriateness or inappropriateness of eradication therapy.
Relationship between HP and functional dyspepsia remains unclear. According to some observations, functional dyspepsia in only 28-40% of cases is combined with chronic gastritis associated with HP. However, between the clinical symptoms considered characteristic of functional dyspepsia and the presence of contamination HP The gastric mucosa has not established any significant relationship: no specific symptoms have been identified that are characteristic of HP-positive patients with functional dyspepsia. And the significance of HP in the development of gastric motility disorders is controversial.
Views on the feasibility of eradication HP in functional dyspepsia and gastroesophageal reflux disease are very controversial. In particular, some researchers believe that eradication HP in functional dyspepsia, as in gastroesophageal reflux disease, is necessary, while others believe that infection HP in patients with reflux esophagitis and chronic gastritis may have a protective effect.
According to some researchers, infection HP in the population is significantly associated with the presence of dyspepsia syndrome and can be "responsible" for only 5% of the symptoms that are considered characteristic of lesions of the upper gastrointestinal tract: eradication helps to reduce the frequency and intensity of dyspepsia, but this does not lead to an improvement in the quality of life of patients. Eradication therapy may be economically justified in functional dyspepsia associated with chronic gastritis in HP-infected patients, but decision makers must be prepared to pay for such treatment.
Taking into account the long-term results of treatment of patients, it was found that eradication therapy for chronic Helicobacter gastritis did not justify the hopes placed on it in eliminating the symptoms of functional dyspepsia. An increase in the level of gastric secretion that occurs in some patients with gastroesophageal reflux disease after eradication HP is a significant factor provoking exacerbation or occurrence of reflux esophagitis. Given the inconsistency in the reports of various researchers, in a wide clinical practice in the treatment of patients with chronic gastritis associated with HP and combined with the syndrome of functional dyspepsia or gastroesophageal reflux disease, anti-Helicobacter therapy should not yet be preferred over antisecretory.
Literature
- Loginov A. S., Vasiliev Yu. V. Non-ulcer dyspepsia// Russian Journal of Gastroenterology. 1999. No. 4. S. 56-64.
- Blum A. L., Talley N. J., O'Morain C. et al. Lack of effect pylori infection in patients with nonulcer dyspepsia// N. Engl. Med. 1998; 339: 1875-1881.
- Brogden R. N., Carmin A. A., Heel R. C. et al. Domperidone. Review of its Pharmacological Activity Pharmokinetics and Theraupeutic Effecacy in the Symptomatic Treatment of Chronic Dyspepsia and as an Antiemetic// Drugs. 1982; 24:360-400.
- Chiral C., Rovinaru L., Pop F. I. et al. Helicobacter pylori and Gastroesophageal reflux Disease — prospective study// Gut. 1999. Vol.45 (Suppl.V.): P.A81.-P.0023.
- Csendens A., Smok G., Cerda et al. Dis. Esoph. 1987; Vol.10: P.38-42.
- Drossman D. A., Thompson W. G., Talley N. J. et al. Identification of subgroups of functional gastrointestinal disorders.// Gastroenterol. Int. 1990; 3:156-172.
- De Groot G. N., de Both P. S. M. Cisapride in the treatment of patients with functional dyspepsia in general practice. Placebo controlled, randomized, double blind study// Aliment. Pharmacol. Ther. 1997; 11:193-199.
- Gilja O. H. et al. Dig. Dis. sci. 1996; 41:689-696.
- Feinle Ch. Interaction between Duodenal Sensitivity to Lipids and Gastric Motility: Its Role in Functional Dyspepsia// Motility. Clin. Perspectives in Gastroenterology. March 1998; 41:7-9.
- Haruma K., Hidaka T. Development of reflux esophagitis after eradication of Helicobacter pylori// Digestive Endoscopy. Jan.1999; 11.1:85.
- Hawkey C. J., Tulassay Z., Szezepanski L. et al. Randomized controlled trial of the effectiveness of eradication of Helicobacter pylori: in patients taking non-steroidal anti-inflammatory drugs; HELP NSAIDs study // Lancet. 1998; 352:1016-1021.
- Iijima K., Ohara S. Increased acid secretion after Helicobacter pylori eradication is the important rick factor of acute duodenitis and reflux esophagitis// Digestive Endoscopy. Jan.1999; Vol.11; #1: 85.
- Kaess H. et al. Klin. Wochenschr. 1988; Vol. 66:208-211.
- Kaise M., Susuki N. Clinical problems occur after Helicobacter pylori eradication in patients with healed peptic ulcer// Digestive Endoscopy. Jan.1999; 11(1): 85.
- Koch K. L. Motility Disorders of the stomach// Innovation towards better GI care. Janssen-Cilag congress. abstracts. Madrid. 1999: 20-21.
- Laheij R. G. F., Janssen J. B. M. J., Van de Klisdonk E. H. et al. Review article: Symptom improvement through eradication of Helicobacter pylori in patients with nonulcer dyspepsia// Aliment. Pharmacol. Ther. 1992; 10:843-850.
- Mario K. Maastricht guidelines for the treatment of non-ulcer dyspepsia: are they applicable in countries with a high prevalence of Helicobacter pylori infection// Russian. Well Gastroent., Hepat., Colorect. 1999.T. U111. No. 3. S. 79-83.
- Mullan A. Eur. J. et al. Clin. Nutr. 1994; Vol. 11:97-105.
- Nandurkar S., Talley N. J., Xia H. et al. Dyspepsia in the community is linked to smoking and aspirin use but not to Helicobacter pylori infection// Arch. Intern. Med. 1998; 158: 1427-1433.
- Sakurai K., Takahashi H. Incidence of esophagitis after H. pylori eradication therapy// Digestive Endoscopy. Jan 1999; 11(11): 86.
- Stanghellini V. Treatment of Dyspepsia// Clinical therapeutics. 1998; 20:D1-D2.
- Stanghellini V. Subgroups, predominant symptoms, dysmotility and hypersensitivity// Innovation towards better GI care. 1. Janssens-Cilag congress. abstracts. Madrid. 1999; 40-41.
- Talley N. N. J. H. pylori as cause dyspepsia: a neu data// GI Therapies. 1998; Issue 3: 1-2
- Talley N. J., Colin-Jones D., Koch et al. functional dyspepsia. A classification with duidelines for diagnosis and management// Gastroenterol. Int. 1991; 4:145-160.
- Talley N. J., Janssens J., Lauristen K. et al. Eradication of Helicobacter pylori in functional dyspepsia: randomized double blind placebo controlled trial with 12 moths fullow up// British. Medical. Journal. 1999; 318: 833-837.
- Hoogerwert W. A., Pasricha P. J., Kalloo A. N., Schuster M. M. Pain: The over looked symptom in gastroparesis// Am. J. Gastroenterol. 1999; 94:1029-1033.
- Colin-Jones D. G., Raczweet B., Bodemar G. et al. Management of indigestion: Message working group// Lancet. 1988; 576-579.
- Moayyedi P., Soo S., Deeks J., et al. Systematic review and economic evaluation of Helicobacter pylori eradication treatment for non-ulcer dyspepsia// BMJ. 2000; 321:659-664.
- Rodriguez-Stanley S., Robinson M., Earnest D.L. et al. Esophageal hypersensitivity may be a major cause of heartburn// Am. J. Gastroenterol. 1999; 94:628-631.
- Delaney B. C., Wilson S., Roalfe A. et al. Randomized controlled trial of Helicobacter pylori testing and endoscopy for dyspepsia in primary care// BMJ. 2001; 322: 898-902.
- Moayyedi P., Feltbower R., Brown J. et al. Effect of population screening and treatment for Helicobacter pylori on dyspepsia and quality of life in the community: a randomized controlled trial // Lancet. 2000; 355: 1665-1669.
Yu. V. Vasiliev, doctor of medical sciences, professor
Central Research Institute of Gastroenterology, Moscow
According to world statistics, functional dyspepsia is the fourth most common diagnosis established by general practitioners and family doctors based on the results of the initial examination of patients. In our country, gastroenterologists began to put it more often, although therapists and family doctors still use the term "chronic gastritis" when making a preliminary diagnosis for patients who complain of dyspeptic symptoms.
This is not correct, because chronic gastritis is a disease with a known morphological basis. At the same time, functional dyspepsia is a diagnosis of exclusion, which requires a thorough examination of the patient to confirm the absence of a morphological substrate for symptoms.
As a rule, functional dyspepsia affects people of working age, more often women. The quality of life of patients is significantly reduced, their working capacity is impaired, they are prone to depressive disorders, which generally predetermines the high medical and social significance of the problem. The task of treating such patients can be more difficult than helping patients with a well-defined organic pathology, for example, peptic ulcer, since with functional dyspepsia there is no usual framework for course therapy; digestive disorders are nonspecific chronic and difficult to correct.
Dyspepsia is a sensation of pain or discomfort localized in the epigastric region, closer to the midline, in the absence of symptoms of reflux (although the patient may also complain of heartburn). Common symptoms of dyspepsia are a feeling of heaviness in the stomach, belching, pain or discomfort, bloating in the epigastric region, rapid satiety, less commonly nausea, and occasional vomiting.
According to modern concepts, the cause of functional dyspepsia is the discoordination of regulatory influences in the brain-alimentary canal system, resulting in a violation of two functions of the gastrointestinal tract - secretory (acid-producing) and motor. A prerequisite for establishing a diagnosis of functional dyspepsia is the absence of an inflammatory reaction of the mucous membranes of the stomach and intestines. Inflammation is a sign of organic pathology.
It is the violation of motor function that most often determines the symptoms of functional dyspepsia. So, insufficient relaxation of the fundus of the stomach in response to food intake causes a feeling of heaviness and early satiety. Dysmotility of the stomach can acquire various forms: arrhythmia (absence of contractions of certain parts of the stomach), tachygastria or bradygastria (accelerated or, conversely, slow contraction), paresis of the stomach with impaired gastroduodenal evacuation.
It should be noted that a violation of the motor function of the stomach always causes dysmotility of the small intestine and biliary tract, since these structures are closely related to each other by the action of local hormones-regulators - cholecystokinin, secretin, etc.
There are three stages in the diagnosis of functional dyspepsia. At the first stage, the doctor must evaluate the complaints, the clinic and the course of the disease according to the anamnesis. Complaints, as a rule, are numerous, they note a decrease in the trophic status, psycho-emotional state; history - experience diet food with the exclusion of certain foods, which, according to the patient, he does not tolerate well. Second phase - general analysis blood, stool for occult blood, test for H. pylori infection. The third stage is fibrogastroduodenoscopy with biopsy and morphological examination to exclude chronic gastritis, ulcers or other organic pathology.
According to unified clinical protocols medical care patients with dyspepsia use non-drug methods of treatment (normalization of the daily routine, diet, psychological correction), as well as medications depending on the presence or absence of H. pylori infection. Patients with Helicobacter pylori infection are shown eradication therapy according to standard schemes lasting 10-14 days. Patients without H. pylori infection are prescribed proton pump inhibitors or prokinetics (depending on clinical variant dyspepsia) for 4 weeks or a combination of these two classes.
There is no indication of probiotics or enzyme preparations in the clinical protocol. Patients with functional dyspepsia do not need these drugs, since they do not affect the course of the disease.
Motilium (domperidone) is a classic and well-studied prokinetic agent that has been widely used in the treatment of patients with functional dyspepsia for more than 30 years. Motilium is the drug of choice for the treatment of patients with symptoms of dyspepsia, which provides fast action directly in the stomach and has a favorable safety profile.
The complex mechanism of action of the drug motilium allows you to directly influence the symptoms of dyspepsia. Motilium increases the tone of the lower esophageal sphincter (this eliminates a symptom such as belching, prevents gastroesophageal reflux), normalizes gastric peristalsis, accelerates the evacuation of gastric contents into the duodenum (relieves a feeling of heaviness, fullness, nausea).
Normalization of gastric motility under the influence of domperidone improves antroduodenal coordination, which has a positive effect on the motor function of the small intestine, the sphincter of Oddi and the gallbladder, helps to restore the physiological processes of evacuation of bile and pancreatic secretion, passage of chyme.
Due to the complex action of the drug motilium, such a symptom of dyspepsia as a feeling of heaviness in the epigastrium, which most impairs the quality of life of patients, is effectively eliminated. The feeling of heaviness, which patients often describe with the words “food lies like a stone in the stomach”, does not go away between meals, and sometimes makes patients artificially induce vomiting in themselves.
Most patients with functional dyspepsia have reduced trophism, so the diet should provide enough energy, plastic material and micronutrients (vitamins and trace elements). In addition, the purpose of diet therapy is to prevent violations of secretion, motility and digestion, improve the psycho-emotional state of patients. This is facilitated by the inclusion in the diet of foods containing the amino acids glutamine, glycine, omega-3 fatty acids.
Patients with functional dyspepsia may not tolerate legumes (contain protease inhibitors), foods rich in indigestible fiber, organic acids, trans fats, prolamin, gliadin (rye, wheat, oats), histamine, tyramine (cheeses, red wine, beer).
Some doctors in patients with complaints of heaviness in the stomach unreasonably use pancreatic enzyme preparations. Exocrine pancreatic insufficiency, which remains the main indication for the appointment of enzyme preparations, develops in conditions of deficiency of about 75% of the volume of digestive enzymes, and it is not as common as functional dyspepsia.
Since functional dyspepsia is caused by impaired gastric motility, it does not apply to such a diagnosis as chronic pancreatitis. Prokinetics, in particular motilium, are first-line agents for functional dyspepsia, since they directly eliminate its cause - a slowdown in the evacuation of food from the stomach into the duodenum.
Enzyme preparations act in the lumen of the small intestine and do not affect the motility of the gastrointestinal tract, but suppress the secretion of the releasing factor cholecystokinin by the mucous membrane of the small intestine, reducing the exocrine function of the pancreas and the motility of the gallbladder. Therefore, the appointment of enzymes for patients with functional dyspepsia is not beneficial.
The differential diagnosis of functional dyspepsia and exocrine pancreatic insufficiency is based on some typical differences in the clinic and course of these diseases. Patients with functional dyspepsia are, as a rule, young people, mostly women, who are prone to depression, self-medication with a variety of diets.
With functional dyspepsia, there are no periods of exacerbation and remission, characteristic of the course chronic pancreatitis. With exocrine pancreatic insufficiency, polyfecal (pancreatic diarrhea) with steatorrhea is usually observed, while with functional dyspepsia, bowel movements are normal.
Compliance clinical protocol treatment of functional dyspepsia, which is based on the use of prokinetics, prevents medical errors, allows doctors to protect themselves from legal prosecution, and most importantly, effectively eliminate the symptoms of dyspepsia, returning patients to the joy of life.
Functional gastric dyspepsia- a symptom complex, including pain or discomfort, feelings of fullness in the epigastric region, early satiety, bloating, nausea, vomiting, heartburn or regurgitation, intolerance to fatty foods, but a thorough examination of the patient does not reveal any organic lesion (peptic ulcer, chronic gastritis, duodenitis, stomach cancer, reflux esophagitis, etc.).
Causes of functional gastric dyspepsia:
1. Psycho-emotional stressful situations (acute and chronic)
2. Nutritional disorders: irregular food intake, change in diet, overeating, abuse of carbohydrates, coarse vegetable fiber, spicy and irritating food
3. Food allergy.
4. Smoking, alcohol abuse.
5. Exogenous factors - high air temperature, high atmospheric pressure, vibration, ionizing radiation, burns, gastrotropic medications(NSAIDs, GCS, etc.).
6. Diseases of other organs and systems (nervous, endocrine, cardiovascular, respiratory, urogenital, hematopoietic), as well as diseases of the digestive system (liver, biliary tract, pancreas, intestines).
Clinical variants of functional gastric dyspepsia:
1) reflux-like- heartburn, sour belching, epigastric pain, retrosternal burning, aggravated after eating, bending over, in the supine position
2) ulcerative- episodic pain in the epigastric region, often occurring on an empty stomach, disappearing after eating or antacids, forcing to wake up at night
3) dyskinetic (motor type)- a feeling of heaviness and fullness after eating, a quick feeling of satiety, belching, flatulence, rarely - prolonged vomiting
4) non-specific- characterized by a variety of multifaceted symptoms, combining the symptoms of three different options
In addition, numerous neurotic manifestations are characteristic: weakness, headaches, irritability, psycho-emotional lability, cardialgia, etc.
To make a “diagnosis of exclusion” of functional gastric dyspepsia, it is necessary to carry out the entire complex of laboratory and instrumental studies in order to exclude organic lesions of the stomach (EGD with mucosal biopsy, radiography with a barium passage, ultrasound of the abdominal organs).
Principles of treatment of functional gastric dyspepsia:
1. Elimination of neuropsychic factors and stressful situations, normalization of relations in the family and at work, a rational mode of work and rest.
2. Rational psychotherapy (including hypnotherapy)
3. Frequent fractional, poor nutrition with the exception of indigestible and fatty foods.
4. Cessation of smoking, drinking alcohol, taking NSAIDs.
5. The use of antacids and H2-histamine receptor blockers (mainly for reflux-like and ulcer-like forms of functional dyspepsia)
6. If a Helicobacter pylori infection is detected in patients with functional dyspepsia, a course of Helicobacter pylori therapy
7. Prokinetics for the normalization of gastrointestinal motility (metoclopramide / cerucal, domperidone / motilium, cisapride / propulsid / coordinatex 5-10 mg 3-4 times a day before meals)
Chronic gastritis (CG)- a disease associated with chronic inflammation of the gastric mucosa, accompanied by a violation of the secretory, motor, endocrine function of this organ.
Etiology of HCG:
1) Helicobacter pylori - a gram-negative bacterium, one of the main causes of chronic hepatitis
2) side effects a number of drugs (long-term use of NSAIDs, etc.)
3) an autoimmune process (at the same time, antibodies to parietal cells that block acid production, as well as antibodies to cells responsible for the production of the internal factor of Castle) are found in the blood
CG classification (Houston, 1994):
1. By etiology:
A) non-atrophic (associated with Helicobacter pylori, hypersecretory, type B)
B) atrophic (autoimmune, type A)
C) chemical-toxic induced (type C)
D) special forms (granulomatous, sarcoidosis, tuberculosis, eosinophilic, lymphocytic, etc.)
2. According to the topography of the lesion: a) pangastritis (common) b) antrum gastritis (pyloroduodenitis) c) gastritis of the body of the stomach
3. According to the severity of morphological manifestations- the severity of inflammation, activity, atrophy, intestinal metaplasia, the presence and type of Helicobacter pylori are assessed (semi-quantitative assessment)
Clinical manifestations of CG:
A) non-atrophic: heartburn, pain in the epigastric region that occurs 30-40 minutes after eating, sour belching, sour taste in the mouth
B) atrophic: nausea, belching, feeling of heaviness in the epigastric region after eating, often diarrhea; signs of B12 deficiency anemia
Objectively: the tongue is covered with a white-yellow coating; with atrophic gastritis - pallor of visible mucous membranes and skin; with superficial palpation of the abdomen in the epigastric region - soreness.
Diagnosis of CG:
1. EGD with mucosal biopsy (minimum 5 pieces) is a mandatory method for diagnosing chronic hepatitis.
2. X-ray of the stomach with a passage of barium - only if a biopsy is contraindicated; signs of chronic hepatitis: smoothing of mucosal folds, impaired evacuation of barium suspension from the stomach (acceleration or deceleration)
3. Intragastric pH-metry - allows you to study the secretory function of the stomach, to conduct an electrometric study of the concentration of HCl.
HCG treatment:
A) treatmentHelicobacterpylori-associated hCG:
1) for the period of exacerbation - diet No. 1 (exclusion of salty, fried, smoked, peppered foods), in the subsequent fried, peppered, smoked dishes are also excluded.
2) eradication therapy - I line (three-component): within 7 days omeprazole 20 mg 2 times / day + clarithromycin 500 mg 2 times / day + amoxicillin 1000 mg 2 times / day or metronidazole 500 mg 2 times / day; in case of ineffective therapy of the 1st line according to the FGDS-control - 2nd line (four-component): within 7 days omeprazole 20 mg 2 times / day + bismuth subcitrate / de-nol 120 mg 4 times / day + metronidazole 500 mg 3 times / day + tetracycline 500 mg 4 times / day.
3) antacids - almagel, gefal, phosphalugel, gastal, maalox, reopan, etc. 1 hour after eating for 10-12 days
4) H2-blockers of histamine receptors - famotidine, kvamatel, ranitidine
5) with severe pain - antispasmodics - no-shpa, papaverine, spasmolin, etc.
B) treatment of autoimmune chronic hepatitis:
1) exclusion of fiber ( fresh vegetables), because it enhances the motor function of the stomach, exacerbates diarrhea
2) if the secretion is not completely suppressed - plantain juice (1 tablespoon 3 times a day), pentaglucid (psyllium elements) - 3 times a day before meals, lemontar 1 tablet 3 times a day, etc.
3) replacement therapy with natural gastric juice - 1 tablespoon 20-30 minutes before meals 3 times a day; 3% HCl with pepsin 3 times a day before meals, acidin-pepsin 1 tab. 3 times a day
4) enzyme preparations: festal, pancreatin, mezim-forte, krion, pancitrate, etc.
B) treatment of drug gastritis:
1) diet No. 1 for the period of exacerbation + cancellation of the drug that caused the gastritis process (NSAIDs)
2) antisecretory drugs: H2-blockers, proton pump inhibitors (omeprazole 20 mg 2 times / day, rabeprazole 20 mg 1 time / day, lansoprazole 30 mg / day)
3) reparants: sea buckthorn oil, solcoseryl, iron and zinc preparations.
ITU: VN with exacerbation of the process 5-7 days.
Rehabilitation: diet, therapeutic mineral waters, phytotherapy, exercise therapy, sanatorium treatment (resorts of Druskininkai, Essentuki, Izhevsk mineral waters, in the Republic of Belarus - "Naroch", "Rechitsa").
Read also...
- Other names: sleepy dope, belladonna, wild berry, wild cherry, rubuha
- Other names: sleepy dope, belladonna, wild berry, wild cherry, rubuha
- Aspartic acid mechanism of action and regimen of administration L aspartic acid chemical properties
- Symptoms and diagnosis of Dupuytren's disease - treatment, surgery and rehabilitation course Mkb 10 Dupuytren's contracture treatment terms