Drug treatment of ovarian cancer. Operational treatment of cancer: efficiency, methods and approaches, localization of the Golden Standard for the Treatment of Officon Oncology
For the treatment of ovarian cancer, surgical, radiation and chemotherapeutic methods are used.
Surgical treatment is considered the main one. Most oncologist specialists are confident that all patients with ovarian tumors should be treated with the help of surgical intervention. This is due to the impossibility of setting the perfectly accurate diagnosis of cancer: if the doctor is mistaken with the determination of the stage of the tumor, then the rejection of the operation can lead to irreparable consequences.
When cancer, one or both ovaries are removed, either carry out a supervised or complete removal of the uterus.
Why with a cancer in one of the ovaries sometimes you have to remove both appendages? The fact is that the danger of the development of a malignant process in the second ovary is very high. After some time, cancer can resume, and the patient will again have to undergo a course of treatment.
Simultaneously with the operation uses treatment with chemotherapeutic drugs. The objectives of such therapy are as follows:
- prevention of metastasis and repeated tumor development;
- impact on the likely residual elements of cancer cells;
- braking of tumor growth;
- facilitate the life of the patient in running cases.
Radiation therapy never applies like independent view Treatment. The problem of irradiation is to provide a high percentage of efficiency of operational and drug impact.
The protocol for the treatment of ovarian cancer is determined only after a careful examination of the patient: the condition of the urinary system, liver is estimated, blood test is carried out. During chemotherapy, blood is examined several times, at least once a week.
In addition, the choice of therapeutic scheme depends on the following circumstances:
- from the presence of concomitant diseases;
- from blood picture;
- on the weight of the patient;
- from histological type of tumor;
- from the process stage.
Surgical treatment of ovarian cancer
Operation is the main link in the successful treatment of cancer tumor. Currently, intervention is carried out using laparotomy - by incision over the pubic zone. Simultaneously with the surgeon operation takes materials for further research. These can be tissue samples or liquid accumulated in abdominal cavity.
- Ouriectomy is resection of one or two appendages.
- Pagierrectomy is an operation that is carried out at the later stages of the development of the tumor when you also have to delete the uterus.
- Extraitation is a complete removal of the uterus with ovaries, a gland and a cervical.
If the tumor strikes only the reproductive system, then the doctor removes the udatki uterus, the nearest lymph nodes, sometimes a worm-shaped process (Appendix).
If the ovarian cancer was invasive, then some elements of the digestive and urinary system also have to be removed.
Immediately after surgery, the patient is prescribed a course of medicines and, in some cases, radiation therapy.
Palliative operations for cancer of the ovaries are carried out when the process is on the running stage, and the patient is not fully cured completely. The essence of palliative treatment is in facilitating the state of the patient and in the maximum possible extension of life.
Radiation therapy
The principle of radiation therapy is in the effects of radioactive rays on the zone of malignant lesion. Rays contribute to the destruction of cancer cells, much easily affecting healthy fabrics.
Most often, irradiation is prescribed during cancer relapse, as well as for palliative treatment, to reduce pain, discomfort and slow down the progression of the process.
Rauchery treatment is carried out in stationary conditions. To facilitate the state of patients, it may be necessary from one to ten sessions, the duration of which determines the oncologist. Simultaneously with the course of radiation therapy, chemotherapy can be taken to fully control the cancer process.
If irradiation is prescribed after surgery, its purpose becomes the destruction of cancer cells, which probably could remain in the body.
In the growth of the tumor in the tissue of the abdominal organs, as well as when the fluid is accumulated, there is no sense in the appointment of radiation therapy, because radioactive rays can have a negative impact on healthy nearby organs.
Treatment of cancer of the ovarian chemotherapy
Chemotherapy is the use of anti-cancer (cytotoxic) medicines for the destruction of the tumor. These medicinal products Inhibit the development of malignant cells. They are introduced into a vein or artery.
It is observed that the ovarian cancer is extremely sensitive to chemotherapy. In many patients, the pathological focus becomes much smaller, and in the early stages of the process, even complete cure may come.
Chemotherapy are used after operational intervention, to prevent the re-growth of the tumor. In addition, special medicines make it possible to reduce the size of the neoplasm before the operation and somewhat reduce the negative manifestations of the disease.
Chemotherapy courses for ovarian cancer are carried out outpatient, for 4-5 months, with minor breaks. Total spend from 2 to 4 courses.
Sometimes preparations are administered directly into the abdominal cavity, through the catheter. This method allows to increase the percentage of women's survival with malignant tumors. However, with intra-abdominal administration, unwanted phenomena may occur, for example, severe pain, the development of infection, diversity of digestive organs.
The most common medicines for ovarian cancer:
- Carboplatin - 100 mg / m² for five days;
- Paklitaxel - 175 mg / m² during the day;
- Topotekan - 1.5 mg / m² for 5 days;
- Cisplatin - 15-20 mg / m² for 5 days;
- Docetaxel - 75-100 mg / m² once, every three weeks;
- Hemcitabine - 1 mg / m² in the first, eighth and fifteenth day every 28 days;
- Etoposide - 50 mg / m² for 21 days;
- Wepzid - 50 mg / m² for 21 days;
- Bevacizumab (Avastin) - 5-10 mg / kg every 2 weeks.
Cytotoxic drugs are almost never prescribed in the form of independent treatment, but only in combination with each other. For example, a combination of taxol + carboplatin with ovarian cancer is called "gold standard" treatment. This combination is less toxic than the combination of cyclophosphane-cisplatin similar to it, but also effective. Taxol with carboplatin provide relatively rapid results and guaranteed 6-year survival of patients.
Doxorubicin, or Kelix, with ovarian cancer, is often used in conjunction with cyclophosphamide or taxanes. At the same time gain toxic action Preparations do not occur. Kelix is \u200b\u200busually administered intravenously (2 mg / ml), and for other drugs, you can choose a different route of administration. For example, oral cyclophosphamide is prescribed in a dosage of 1-2 mg / kg per day.
Avastin with ovarian cancer is applied relatively recently. This is one of the new preparations based on Bevacizumab, oppressing the development of a malignant tumor. Avastin is administered only by intravenous drip. Another version of the introduction, including intravenous jet, is prohibited.
Another of the most popular antitumor drugs - refdot - is a factor of necrosis of tumor tissues (thymbosin α-1). This is a fairly strong cytostatic and cytotoxic agent that has a minimum amount. side Effects. Nevertheless, the refrigeratot for cancer of the ovaries is not so often: it is usually prescribed for the treatment of breast cancer.

In addition to antitumor drugs, often doctors prescribe immunomodulators - these are medicines that support immune system man in a "battle" condition. The use of immunomodulators is still disputes in the ranks of medical professionals. Some of them consider such drugs useless in oncology, while others are confident in their need. So, it is believed that the most common means of Roncolekin with ovarian cancer increases antitumor immunity, which significantly increases the efficiency of chemotherapy. In addition to Roncolekina, such medical preparations such as Timalin, Mielopid, Betaleikin and Interferons have such actions.
Thermoperfusion with ovarian cancer
Thermoperfusion is one of their treatment options for oncology, which implies the thermal effect on the tissue. High temperature damages the protein structure of cancer cells without affecting healthy sitesthat allows you to noticeably reduce the size of the neoplasm. In addition, thermotherapy increases the sensitivity of tumor tissues to irradiation and chemotherapy.
The essence of thermopyrus is to process the ovaries and nearby organs that were subjected to cancer, a warm antitumor agent (up to 44 ° C), which significantly increases the efficiency of its action.
In addition to antitumor action, this method It has a number of side manifestations. These are swelling, increasing thrombosis, bleeding, pain. Over time, these symptoms take place independently. Dyspeptic disorders can occur less often, as well as exacerbation chronic diseases of cardio-vascular system.
Currently, active clinical trials of thermotherapy are carried out. This is done to increase the efficiency of the method and eliminate its possible negative consequences.
Treatment of ovarian cancer by folk remedies
Is it possible to cure a cancer tumor with folk recipes? The question is controversial. The vast majority of specialists in traditional medicine Do not welcome the application folk remediesMoreover, in the form of independent treatment. Attempts to cure the tumor can independently lead to the aggravation of the process, and the precious time to start timely treatment May be lost.
Nevertheless, a lot of recipes are known, the authors of which promise to get rid of ovarian cancer. We invite you to familiarize yourself with some of them.
- Known active application Mintage in the problems in the sexual sphere: for example, with strong menstrual bleeding, with painful climax, etc., the mint is successfully used with the ovarian cancer: it is customary to take the tea from flea mint for three times a day. During treatment, you can dialect by the same solution. To prepare such tea, you need to brew 20 g of mint leaves in 500 ml of boiling water and insist from 2 to 3 hours.
- Linen oil and flax seed with ovarian cancer is used very often. Oil dosage ranges from 1 tsp. up to 1 tbsp. l. in the morning and in the evening. You can take it in the form of capsules that are sold in pharmacies. To do this, you need to drink at one time from 10 to 14 capsules. Linen seed is used in the amount of 3 tbsp. Spoons mixed with 200 ml of water. Such a "cocktail" needs to drink three times a day, minimally for one month.
- Good reputation in the fight against cancer disease It has Boligols - it is used to treat many malignant tumors. Boligols with ovarian cancer (especially in a complex with other techniques) can lead to a positive result. The tincture of this plant should be accepted with a gradual increase in dose: starting with 1 drops for 200 ml of water 1 time per day before meals, bringing up to 40 drops. Simultaneously with the amount of drug, the amount of water increases (for every 12 cap. + 50 ml). After reaching 40 cap. The dosage is reduced in the opposite direction, 1 drops per day. The amount of water is also reduced by 50 ml every 12 cap. The duration of such treatment is as much as it is necessary for complete healing.
- Many consider the first medicine from malignant tumors. Ordinary Oats. The infusion of oats in the cancer of the ovaries is prepared very simply: one glass of oatmeal is falling asleep into an enamelled container and poured 1000 ml of water, bring to a boil and boil on a small fire for about 20 minutes. After that, remove from the fire and insist in a warm place for at least 2 hours. The decoction is filtered and divided into three receptions. They drink 30 minutes before reception of food three times a day. Cooking a decoction in advance for several days is not recommended, it is better to take fresh.
No one excludes efficiency folk treatment. However, before using such methods, consultation with an oncologist must be mandatory.
Treatment of cancer of ovarian stages
The treatment of ovarian cancer at the 1st stage is most often carried out only by operational intervention. At the same time, the surgeon makes hysterectomy, double-sided salpingooforectomy and excision of the gland. In addition, during the operation, materials for biopsy and peritoneal liquid washing was taken. In most cases, the 1st stage does not require additional treatment, except for surgical.
The treatment of ovarian cancer at 2 stages is carried out by analogy with the first stage, but is additionally appointed radiation therapy Or systemic chemotherapy, which implies the use of platinum-based medicines together with alkylating drugs or paclitaxel.
The treatment of ovarian cancer at 3 stages require a combination approach, which combines the operation and mandatory course of chemotherapy. It is often used intraperous version of chemotherapy, using cisplatin and various combinations with it.
The treatment of ovarian cancer at 4 stages is more complex and less optimistic. The main methods of impact on such a tumor are:
- citics Surgery is the removal of one main affected part of the cancer neoplasm, which cannot be completely removed;
- systemic chemotherapy - the use of cisplatin or carboplatin in combination in taxanes or other similar drugs;
- consolidating or supportive treatment is the appointment of more than six consecutive chemotherapy courses, which allows you to move the development or to completely avoid relapses. Such treatment is most suitable for patients with chemical sensitive tumors.
Treatment of ovarian cancer in Israel
Treatment of cancer tumors in Israel is carried out in modern high-tech medical centers, which are equipped with special profile offices of female oncology therapy. The treatment is engaged simultaneously a number of specialists - this is a surgeon-oncologist, a gynecologist-oncologist, a chemotherapist-oncologist and a radiologist. Most Israeli medical institutions represent eminent professors known all over the world.
It is important and the presence of the most modern diagnostic and therapeutic equipment in clinics. The development of medicine in this country is paid to a lot of attention, including priority financing from the state. Therefore, medical centers, as a rule, have a powerful diagnostic base, thanks to which the complex surveys can be carried out literally in a few days.
Chemotherapeutic treatment in Israel is based on the use of the newest medical drugs developed according to the latest clinical studies.
For foreign patients, a coordinator is always provided, which owns the necessary language.
When admission, the patient must undergo a mandatory examination, which when the ovarian cancer can do about $ 6,000. Surgical intervention costs about $ 20,000, and one chemotherapeutic course is about $ 3,000.
Treatment of ovarian cancer in Germany
In Germany exists special program According to advanced technologies in the daily practice of the oncological clinics. It is connected with insufficient early diagnosis Cancer tumors.
It is worth saying that the doctors in German medical institutions are especially pedantic and highly qualified, and the equipment of the clinics is presented by the latest technology.
For each case and each patient is always assembled by a consultation, which determines the individual therapeutic approach.
The most common standards for the treatment of ovarian cancer in Germany are:
- surgical system "Da Vinci" (remote robotoshurgery);
- radioshurgery "Cyber-knife system";
- internal radiation impact on the tumor;
- ultrasonic ablation method;
- treatment with monoclonal antibodies.
The surgical operation in Germany can do about 3,000 to $ 10000. The price for one course of chemotherapeutic treatment is from 10,000 to $ 15,000.
New in the treatment of ovarian cancer
- In the United States of America, developed a scheme for the treatment of ovarian cancer with photodynamic therapy. Development is based on the fact that the cancer tumor is detected in most cases only when metastases begins to other organs. After that, the operation and chemotherapy do not have the necessary effectiveness. Therefore, a new treatment method was invented, which is called photodynamic therapy. The patient is proposed to adopt a special preparation - phthalocian, which produces active oxygen, capable of destructively act on the structures of cancer under infrared rays. In addition, genetic therapy is prescribed, which reduces the degree of cell protection against active oxygen. This therapeutic method can be combined with surgical treatment, which reduces the likelihood of intoxication of the body.
- In the UK, developed a new revolutionary antitumor agent of Olaparib. purpose this drug - Extend the life of patients with ovarian cancer, at least five years. Olaparib tests are currently being carried out, and in a short time this means will be affordable for treatment.
Rehabilitation after the treatment of ovarian cancer
After the treatment of ovarian cancer, a number of side effects and exacerbations may arise, which must be removed or soften their current. The rehabilitation scheme will appoint a doctor.
There are several options for rehabilitation therapy, which can be applied with a sufficient degree of efficiency.
- Treatment with supporting drugs:
- antiwheat medications - Zofran, Ativan, etc.;
- laxative medicines - Duhalak, etc., which are prescribed against the background of the corresponding diet;
- hormonal agents are medicines that normalize the hormonal background of women after removing two ovaries;
- drugs-immunomodulators - interleukin, etc.
- Psychological treatment:
- selection by specialists of a certain eating diet and exercise of the exercise
- attracting social care services for patients;
- consultation of the psychotherapist;
- communication with patients who suffered a similar pathology.
- Physiotherapeutic treatment, swimming and rehabilitation gymnastics.
Postoperative treatment by folk methods
Folk remedies Even at the postoperative stage should be used only after approval by the oncologist. It is necessary to consider that many drugs have contraindications for reception.
- The boring uterus tincture: 100 g of chopped grass pour 500 ml of vodka and insist 14 days in a darkened place, sometimes stirring content. To drink 1 tsp. 4 r. / Day. Duration of reception - up to 4 months in a row.
- A decoction or tincture of the Golden Usa: thoroughly crushed the ground part of the plant, pour boiling water and cook a quarter of an hour, after which it is filtered and cool. The decoction take 100 ml three times a day, and the tincture on alcohol - 1 tbsp. l. in a glass of water.
- Freshly squeezed beet juice, spent on one hour: drink, starting with 50 ml, gradually increasing the dose to 0.5-1 l per day.
- Infusion of hop cones: Throw dry cones to the state of the powder. Two teaspoons of this powder pour 200 ml of boiling water and insist for 3 hours. Drink to eating 50 ml three times a day.
Treatment of ovarian cancer recurrences, as well as their prevention, is carried out by such folk methods:
- infusion of Celenee with calendula: Stir the raw material in equal shares and pour 200 ml of boiling water (you can brew in the thermos), leave for 2 hours. Take 100 ml 3 p. / day before meal;
- spitolis alcohol tincture (sold in pharmacies): take 30 drops / day.
The treatment of ovarian cancer is most effectively in the early stages of tumor growth. With the further distribution of the malignant process, the disease forecast becomes much less optimistic.
anonymously
Good evening, my mom is ovarian cancer 3 stages, as a result of which ascites developed. They went to the Oncological Hospital No. 62 (Krasnogorsk district). They made laparoscopy, removed 8 liters (!) Liquid, said that there are metastases on the gland and the abdominal cavity, prescribed 3 chemotherapy (paclitaxel + carboplatin) to operation and 3 more after. We do not know what to do. Help me please!! Is it worth starting to make chemistry here or go for treatment in Israel (acquaintances advise to go there)? We are afraid that chemistry will make it wrong that the equipment in the hospital is not the most newest (which could prevent accurate diagnosis). How to help us ... Help, I ask! ...
Good day. The scheme that doctors appointed is called the "gold standard" of chemotherapy during treatment, especially how they shared the scheme (3 - Operation - 3). In this situation, a lot depends on the cellular structure of cancer, from general status Patients, accommodation pathology, age, etc. The chance of radical cure is very low in such a stage, but it is. If you have the opportunity and the condition of your mom will allow in the shortest deadlines to contact the Israeli clinic, then, of course, try. But 100 percent guarantees will not give you anywhere. And if they start, for example, from 11/14/11, and in the resolon it will begin with the beginning of December, it should not be thoughtfully, it is necessary to start here, since every day in the account. If you are writing questions, I will try to help you. Sincerely, Lisaev D.A.
anonymously
Thank you very much for your reply. Today, Mom made first chemistry. Sorry, but you can find out one more .. There is a break between chemotherapy courses for 3 weeks. Will it be possible during this time to go to the Israeli clinic and repeat the examination? And, perhaps, to spend the operation itself already there. I just want to check everything as much as possible. And they said, the right treatment appointed us here. Began chemotherapy in Moscow, because we do not want to waste time. Tell me, how do you think it will be the most faithful, please ..
Citation:Kozachenko V.P. Treatment of ovarian cancer patients // RMG. 2003. №26. P. 1458.
Russian oncological science Center them. N.N. Blokhina Ramne
R Ak ovarian occupies 7th place in frequency, accounted for 4-6% of the total number of malignant tumors in women. According to Mair (International Cancer Study Agency), every year more than 160 thousand new ovarian cancers are registered in the world. And more than 100 thousand women die from malignant tumors of this organ. IN Russian Federation Every year ovarian cancer is detected by more than 11 thousand women. Over the past 10 years, there has been an increase in the disease by 8.5% in the country. In 2001, 11,788 new cases of ovarian cancer were registered in Russia, 7,300 patients died.
In economically developed countries of the world, ovarian cancer has the most high rates Mortality among all malignant gynecological tumors, which is primarily associated with the late diagnosis of the disease. Mortality of cancer of ovarian cancer In the first year, after establishing a diagnosis, 35% reaches. According to the consolidated data of population cancer registers of Europe, the annual survival rate of ovarian cancer is 63%, three-year-old - 41%, five-year-old - 35%. The classification of ovarian cancer is presented in Table 1.
The risk factors for the occurrence of ovarian cancer include: the absence of pregnancies and childbirth, the irrational use of substitution hormone therapy, hormonal medicia treatment infertility, hereditary factors (the presence of cancer cases of ovarian in the family).
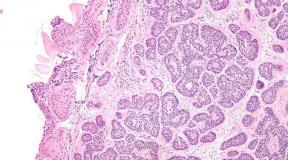
The testing of the tumor is carried out on the basis of the data of the clinical examination, the results of the surgical intervention and histological examination of the biopsies obtained during the operation from various sections of the abdominal cavity. The correct definition of the stage of the tumor process makes it possible to determine the optimal tactics and improve the results of treatment.
Significant difficulties arise in determining the degree of prevalence of the malignant process, especially when initial stages Diseases. In patients with malignant tumors of ovaries I-II stages, at a focused study, metastases are found in the retroperitoneal lymph nodes of various localities (up to 30%). In 28% of patients with the estimated I stage and in 43% of the alleged II stage of the disease are set up later stages of the process. Difficulties of detection of metastases in the retroperitoneal lymph nodes are explained by the fact that retroinchenously, only in the para -orthal zone there are from 80 to 120 lymph nodes, Moreover, each of them can be amazed by micrometastasis. The lymphatic nodes affected by tumor can be not increased, density consistency, freely or relatively shifted. Therefore, 23% of ovarian cancer patients have relapses, although they assumed the early stages of the disease.
Patients with malignant neoplasms of ovarian apply 3 main treatments: Surgical, medicinal and radial.
Systemic drug therapy is an integral part of therapeutic process for the overwhelming majority of patients suffering from ovarian cancer. Almost only in the case of highly differentiated tumors 1a, in the stages it can be limited to operational intervention, which provides a 5-year survival rate of 90% or more. With the same stages with the presence of high-risk signs of recurrence in 35-60% of patients after surgical treatment, relapses arise, which makes it necessary to carry out adjuvant drug therapy to the patients of this group. Starting with 1C stage, due to the deliberate nerakality of surgical treatment, all patients showed the conduct of induction chemotherapy. The risk assessment criteria for recurrence are shown in Table 2.

If there are at least one of the above signs of high risk recurrence, the process should be considered as prognostically unfavorable. In addition, it is known that serous adenocarcinomas are associated with an unfavorable forecast, while endometrium tumors have the best forecast, and mercinal and light cells occupy an intermediate position.
Oncogynecologists in practice are rarely limited to operational intervention. Even at the very early stages and high degree Differentiations of the tumor they prefer "just in case" carrying out preventive chemotherapy. The reason is that even patients with a favorable outlook most often during the operation, the biopsy of the retroperitoneal lymph nodes, the biopsy of the peritoness and washed from it, which does not allow properly stood the tumor process.
Treatment of patients with malignant ovarian tumors follow , usually, start with surgery in order to maximize tumor mass removal . At the same time, the stage of the tumor process is determined. The operation is to remove the uterus with appendages and large glands. Required a thorough examination of the abdominal cavity with biopsy changed the peristine plots, cytological research Aspirates and wasches from the abdominal cavity.
Survival of patients increases with maximum removal of tumor masses during surgery. Five-year-old unqualified survival of cancer patients IA and II stages with purely surgical treatment It is 90%, not differing significantly from the results of combined treatment, at which chemotherapy was additionally used. To increase the survival of patients with other stages of malignant ovarian tumors, the use of adjuvant chemotherapy is obligatory.
In the treatment of patients with common ovarian cancer the generally accepted method is systemic chemotherapy . Since the cytiratement operation is not radical, chemotherapy should be started, it is possible to quickly after operation - usually 10-12 days. When prescribing combined pay-containing modes, the volume of chemotherapy in this category of patients can be limited to 3-4 courses. The elderly patients as adjuvant chemotherapy can be recommended by Melfalan monotherapy at a dose of 0.2 mg / kg / day in 1-5 days every 28 days, 6 courses.
Chemotherapy of the first line The first line standard induction chemotherapy
(under the IC-IV stages) are derivatives of platinum and combinations based on them, which significantly improved the immediate and remote results of treatment compared to the free modes, especially in patients with small size residual tumors.
Cisplatin - one of the most active drugs For the treatment of ovarian tumors. An objective antitumor effect is observed in 32% of patients who previously obtained chemotherapy with chlorohythylaminamins or doxorubicin. When using cisplatin in patients who had not previously obtained chemotherapy, an objective effect was observed in 60-70% of cases, of which 15-20% complete, and 5-year survival was 6%. Unfortunately, combinations with the inclusion of cisplatin are poorly carried by patients due to the pronounced nausea and vomiting, frequent development of nephro- and neurotoxicity. That is why the replacement of cisplatin is promising for less toxic carboplatin. Both drugs have approximately equal effective in the treatment of ovarian cancer, if the doses of two cytostatics are taken in the ratio of 4: 1 (i.e., cisplatin at a dose of 100 mg / m 2 is equal to the antitumor efficacy of carboplatin at a dose of 400 mg / m 2).
Several randomized studies were conducted, in which the effectiveness of combinations with the inclusion of these two platinum derivatives was compared. In all studies where carboplatin was used at a dose of 300 mg / m 2 and higher in combination with other cytostatics (cyclophosphamide, doxorubicin), approximately equal effectiveness in comparison with such with the use of a combination based on cisplatin. In this case, the regimens with the inclusion of carboplatin are transferred to the patients much easier due to the smaller frequency and severity of nausea and vomiting, neuro and nephrotoxicity.
The main problem when using combinations with the inclusion of carboplatin is a more pronounced myelosuppression that causes to reduce the doses of drugs or increase the intervals between the courses, which adversely affects the results of therapy. Meanwhile, the data obtained show that the combination of carboplatin + cyclophosphamide is a circuit of choice in patients with common ovarian cancer. It is recommended to use carboplatin at a dose of 300-360 mg / m 2 and cyclophosphamide 500 mg / m 2 every 3-4 weeks.
Carboplatin . Carboplatin is a second-generation preparation from a group of platform-containing. In contrast to its predecessor, the cisplatin carboplatin has less nephrome and neurotoxicity, the ability to cause nausea and vomiting. Basic by-effect Carboplatina is the oppression of blood formation. The frequency of objective effects when using carboplatin in previously treated patients varies from 9 to 32% and on average is 24%. In three randomized studies in previously attacked patients, it was proved that carboplatin at a dose of 400 mg / m 2 is equivalent on the antitumor activity of cisplatin at a dose of 100 mg / m 2 and at the same time less toxic in all respects, except for the oppression of blood formation.
Widespread use of the combined chemotherapy method of the 1st line according to the scheme: Cisplatin 75 mg / m 2 (or carbopine AUC-7) and cyclophosphamide 750 mg / m 2 with 6 courses at intervals 3-4 weeks.
Since the total excretion of carboplatin from the body is lower in patients with impaired kidney function, on the one hand, and platelet levels in blood tests after intravenous administration of carboplatin correlates with an area under a pharmacokinetic curve (AUC), on the other hand, to prevent myelosuppression was developed and selected formula Calverta:
Dose (mg) \u003d (necessary AUC) X (CGF + 25),
where CGF is the speed of glomerular filtering.
According to the calcaret formula, the dose of carboplatin is calculated in mg (and not in mg / m 2), allowing the correct selection of the dose of carboplatin as in patients with a reduced kidney function and in patients with high values Renal clearance.
The flushing filtration rate corresponds to creatinine clearance, which can be designed by Cokroft's formula:
(K (coeff.) X (140 - age) x Weight per kg) / (Creatine serum),
where k \u003d 1.05 for women, K \u003d 1, 23 for men.
Thus, the inclusion of platinum derivatives in the modes of induction polychimotherapy during ovarian cancer today is mandatory.
However, in Russia, such patients are often still prescribed by free combinations, which cannot be considered adequate.
Pronounced nephrome and neurotoxicity, as well as ectopicity, are a significant disadvantage of cisplatin. Along with cisplatin, in patients with ovarian cancer equally, the platinum derivative of the second generation - carboplatin can be used, in the spectrum of the toxicity of which myelosuppression prevails. Equivalent doses of carboplatin (4: 1 in a cisplatin ratio) make it possible to provide approximately equal effectiveness with less toxicity, with the exception of hematological. Calculation of the dose of carboplatin using the calcult formula (AUC 5-7) ensures the optimal ratio of the efficiency and toxicity of treatment (Table 3).

The most popular combinations based on derivative platinum are PC. (Cisplatin + cyclophosphamide 75/750 mg / m 2) and SS (Carboplatin + cyclophosphamide AUC \u003d 5/750 mg / m 2).
Recently, the standard diagram of chemotherapy I line is the use of platinum and taxanov derivatives. Among the latest most studied and widely used preparations of Paklitaxel and Docetaxel.
Paklitaxel Represents drug vegetable originderived from the bark of tees. The drug stimulates the polymerization of tubulin and the formation of non-functioning microtubules, which leads to a violation of the mitosis process and intracellular transport and, as a result, the death of the tumor cell. When conducting the second phase of clinical trials, the effectiveness of paclitaxel was studied as a second or third line chemotherapy in patients with ovarian cancer who received platinum preparations. On a large number of patients, it was shown that paclitaxel in monochimotherapy mode is effective drug In the treatment of this prognostically unfavorable group of patients. The frequency of objective effects lasting from 3 to 6 months is 20-36%.
It seems promising the use of paclitaxel for intraperitoneal administration. The large molecular weight and dimensions of the Paklitaxel molecule determine the slow absorption of the drug into the blood when it is introduced intraperitoneally. In the abdominal cavity is created high concentration The drug (more than 100 times higher than in plasma in intravenous administration), which is preserved for 5-7 days. A single dose for intraperitoneal administration of paclitaxel is 60 mg / m 2. The drug is recommended to introduce weekly for 3-4 weeks. The intraperitoneal administration of paclitaxel can be used to carry out induction chemotherapy of patients with an optimally performed cytoteducleizage operation, when the dimensions of tumor formations do not exceed 0.5 cm, as well as chemotherapy in the second line in patients with minimal manifestations of the disease after induction chemotherapy.
Docetaxel also has high antitumor activity. In particular, its effectiveness in combination with platinum derivatives during induction therapy is 74-84%. It is noted that combinations with the inclusion of docetaxel have less neurotoxicity.
Compliance with the optimal intensity of chemotherapy, allowing to balance the toxicity and effectiveness of treatment, is an important factor in successful treatment, along with right choices medicinal combination. An unreasonable decrease in the number of courses and / or doses of chemotherapy, as well as an increase in intervals between courses inevitably leads to a deterioration in the results of treatment.
A retrospective analysis of numerous work has shown that with an increase in cytostatic doses in the modes of combined chemotherapy or dose of cisplatin during monotherapy, immediate and remote treatment results are improved. However, the correlation "dose-effect" exists in the range from 15 to 25 mg / m 2 / week. (or from 45 to 75 mg / m 2 1 time in 3 weeks), and further increase in the dose does not lead to improved treatment results.
Compliance with the optimal periodicity of treatment is an important component of the part of successful drug therapy. . The majority of chemotherapeutic regimes used in the ovarian cancer include the interval between courses equal to three, less often - four weeks. An increase in the interval may and should be carried out in accordance with clear medical testimony. Most frequent cause Increasing the interval between courses are signs of toxicity, most often - retained by the time the next neutro- and / or thrombocyting cycle began, which is more characteristic of combinations with the inclusion of carboplatin. It is appropriate to recall that the absolute number of neutrophils, equal to 1.5 x 10 9 / l, and platelets, equal to 100 x 10 9 / l, is sufficient to carry out the next course of treatment.
When using standard reduction modes, doses are usually not required, with the exception of serious hematological toxicity (leo and / or thrombocytopenia III-IV degree), complicated by fever and / or hemorrhagic syndrome, which is more often observed when using carboplatin in doses AUC \u003d 6 , 5-7. The phenomena of nephro- and neurotoxicity, as a rule, do not reach pronounced and do not require dose correction.
The right choice of medicinal regime and compliance with the basic principles of chemotherapy makes it possible to obtain an objective antitumor effect in 70-80% of patients with an average duration of remission up to 12 months.
Chemotherapy of the second line Five-year survival of ovarian cancer III Stages It is 20-25%, and IV does not exceed 10%. Despite the disappearance of all signs of the disease, the overwhelming majority of patients in the first 2-3 years after the end of the chemotherapy of the first line comes the progression of the disease, mainly due to the appearance of intra-abdominal metastases. All these patients need to carry out chemotherapy of the second line.
Chemotherapy of the second line allows you to control the symptoms of the disease in most patients, including with tumors resistant to platinum derivative, increase the duration of time to progression and total life expectancy in patients with high sensitivity to platinum, but cannot lead to curable. Therefore, for the overwhelming majority of patients, chemotherapy of the second line is only a palliative character.
Often, in patients with ovarian cancer, the appearance of symptoms of progression of the tumor process precedes an increase in the level of CA-125. It is known that CA-125 is a non-specific marker for ovarian cancer, its increase can be due to the products of chronically inflamed mesothelium of the peritoneum after the previously performed operation and chemotherapy of the first line. It is this circumstance that sometimes causes a moderate persistent presence or an increase in the SA-125 level shortly after the end of treatment in the absence of any signs of the disease. In the case of slowly current tumor progression, the interval between the level of Case-125 and the appearance of other symptoms of the disease can be several months, and sometimes even years.
According to supporters of early beginnings of chemotherapy, treatment with minimal (subclinical) volumes of tumor mass has large chances of achieving a clinical effect. The opponents argue that the chemotherapy of the second line is palliative and its conduct in patients with the absence of symptoms only wishes the general condition due to toxicity without any influence on the disease forecast.
The solution to the question of the start of chemotherapy with increasing CA-125 should take into account the opinion of the patient after its conversation with the doctor, for the patient's emotional alarm is often an increase in SA-125 is the main reason for the start of therapy.
The emergence of signs of the disease after reaching full regression or growth of tumor chemotherapy used after the first line of the first line of the first line - absolute signs Progressions requiring chemotherapy in the second line. In the event of a relapse of the disease, the question may be raised about the feasibility of performing operational intervention. However, very often when performing an operation, in addition to the local recurrence, there are subclinical disseminations in the abdominal cavity.
The effectiveness of chemotherapy of the second line depends on the duration of the interval between the end of the chemotherapy of the first line and the occurrence of the progression of the disease. Than he is longer, the greater the chance of obtaining an antitumor effect upon subsequent treatment. The presence of a relapse of the disease, potentially sensitive to platinum derivative, implies compulsory inclusion in the chemotherapy of cisplatin or carboplatin. therefore it is possible to carry out chemotherapy of the second line by the same scheme that was used earlier at the first line. , or a combination of platinum derivative with a new antitumor drug. Currently, even for patients sensitive to platinum derivatives, it has not been shown that combination chemotherapy has advantages over monotherapy only with cisplatin or carboplatin.
Set antitumor agentsUsed to conduct chemotherapy in the second line is unusually large, which, rather, indicates that none of them allows you to achieve long-term remissions in most patients. The effectiveness of their use ranges from 12 to 40% with an average life expectancy of 9-12 months.
Most often as chemotherapy second line used paklitaxel If it is not used when conducting the first line. Study of various administration modes ( motherwise dose 175 and 135 mg / m 2, 3 and 24 hours infusion) showed that optimal from the point of view of efficiency and toxicity, as well as ease of use, is the dose of drug 175 mg / m2 for 3 hours. In patients whose tumors are resistant to cisplatin, conducting the second line of chemotherapy Paklitaxel makes it possible to achieve an antitumor effect in 20% with a medium life expectancy of 12.5 months. The use of docetaxel in a dose of 100 mg / m 2 for 1 hour with the ovary tumors resistant to the action made it possible to achieve effect in 36% of patients with an average duration of remission 5 months.
Topotekan (Hickin) - The drug from the group inhibitors of topoisomerase I is also widely used to carry out chemotherapy of the second line, the frequency of the antitumor effect in patients with platinum derivatives of the ovarian tumors was 20%, while with a 14% resistant to cisplatin - 14% appointing topotecan in a dose 1 , 5 mg / m 2 V / c for 5 days.
Etoposide, taken inside at a dose of 50 mg / m 2 for 14 days, was effective in 27% patients with tumor cell resistance to platinum derivatives and in 34% stored sensitivity. Liposomal doxorubicin in 82 patients with the progression of the disease after conducting chemotherapy of the first line of platinum derivatives and taxanes allowed us to achieve an objective effect in 27% of patients with an average life expectancy for the entire group of 11 months. .
When appointing a Vinorelbina in a dose of 25 mg / m 2 weekly to carry out chemotherapy of the second line in 24 patients whose tumors were resistant to platinum derivatives, the frequency of the objective effect was 21%.
Gemcitabine is a perspective drug for conducting chemotherapy of the second line. In the treatment of 38 patients with progression after applying a combination of platinum derivatives and taxanes by a hemcitabine at a dose of 1000 mg / m 2 1st, 8th and 15th days every 4 weeks, an objective effect was noted in 15% of patients. Oxaliplatin is a new platinum derivative, which has demonstrated the absence of cross-resistance with cisplatin and carboplatin. This was the basis for studying the effectiveness of oxalyplatin in patients with ovarian cancer, resistant or refractory to platinum derivatives. In the treatment of 34 patients, the frequency of the objective effect when appointing oxaliplatin was 26%.
The unsatisfactory results of the treatment of patients with malignant neoplasms of ovaries make it necessary to combine the efforts of surgeons, chemotherapists and radiologists to develop new programs and treatment methods.
Literature:1. Malignant neoplasms in Russia and the CIS countries in 2001 are ed. M.I. Dodavdova and E.M. Acel. Medical informative agency, 2003, p.293.
2. Eadson D.F. et al. // am j genet. - 1995; Vol.56, p.263-271.
3. Plentl F.V., Friedman E.A. Lymphatic System of the Female Genitalia. Philadelphia: Saunders, 1971.
4. Burghard E. et al. // Am J Obstet Gynecol., 1986; Vol.155, p.315-319.
5. Tulundin S.A. Ovarian cancer: yesterday, today, tomorrow // Materials of the conference "Modern trends in the development of drug therapy of tumors". - M., 1997, p.66-70.
6. Tulundin S.A. Ovarian cancer. - M., 1996, p.63.
7. Gruppo Interegional Cooperativo Oncologico Ginecologia. Randomised Cyclophhamide / Cisplatin and With Cyclophosphomide / Doxorubicin / Cisplatin in Advanced Ovarian Cancer // LanCet. - 1987; Vol.2, p.353-359.
8. Alberts D.S. et al. // j clin oncol. - 1992; Vol.10, p.706-717.
9. Swenelon K., Pater J.I. // seminars in oncology. - 1992; Vol.19, P.114-119.
10. Gorbunova V. et al. // Proc ASCO. - 2000; Abstr.1536.
11. Kennedy A.V. et al. // Proc ASCO. - 2000; Abstr.1563.
12. Levin L., Hryniuk W. // J Cli Oncol. - 1987; Vol.5, p.756.
13. Levin L. et al. // J Natl Cancer Inst. - 1993; Vol.86, p.17-32.
14. McGuire W.P., Ozols R.F. // seminars in oncology. - 1998; Vol.25, p.340-348.
15. Kudelka A.P. et al // j clin oncol. - 1996; Vol.14, p.1552-1557.
16. Muggia F.M. et al // j clin oncol. - 1997; Vol.15, p.987-993.
| "After numerous clinical studiesThe leading experts were recognized that the "gold standard" in the treatment of ovarian cancer is a taxol diagram of 175mg / mg in the form of 3-hour infusion and carboplatinis 5-7.5 every 3 weeks. " Prof. Borisov VM. "Pyccic Medical Journal", Volume 9, №22, 2001 |
"Taxol in combination with cisplatin or with carboplatin is one of the most effective modes of induction chemotherapy in patients with disseminated ovarian cancer" |
| "Currently, the taxol is a non-component of the combined chemotherapy of ovarian cancer, preferably included in the first line of therapy, and in patients who received other chemotherapy used as a second line" Prof. Translator NL. "Taxol B. clinical practice", Under Reduna. Translator, p. 8, 2001 |
"There are convincing visual data of the third phase, two large randomized clinical trials confirming that taxol is a cisplatin-new standard mode for treating patients with common ovarian cancer" |
| « Intravenous administration Carboplatina and taxi is recommended as postoperative chemotherapy mode for newly diagnosed patients with II-IV stages of epithelial cancer of ovaries " Covens A: Gynecologic oncology 85,71-80 (2002) |
Ovarian cancer: randomized GOG 111 study
Ovarian cancer of the III-IV stage suboptimal resection [< 1 см ]M.J. Piccart et al, Journal OF The National Cancer Institute, Vol. 92, No. 9, may 3,2000
OUTPUT:
Combination Taxol + Cisplatin statistically reliably exceeds the combination of cyclophosphane + cisplatin by indicators:
6-year survival
(M.j. Piccart et al., Materials ESMO 2002, Abstra. 395, p. 109)Taxol and carboplatin combination
Considering the nephrotoxicity, dysotoxicity and neurotoxicity of cisplatin, subsequently studied studies of the effectiveness of the combination of taxi and carboplatin. As a result of these studies, equal treatment efficacy was demonstrated, but significantly smaller toxicity of this combination was demonstrated. (Prof. Borisov V.I. "Russian Medical Journal", Tos, No. 22, 2001)
Results of randomized studies with common ovarian cancer
Taxol + Cisplatin compared to a combination of taxol + carboplatin
(Gorbunova V.A. "Taxol 6 Clinical Practice" edited by Translator, p.172., 2001)
¦ Treatment of ovarian cancer
Treatment of ovarian cancer
Development Stage cancer of ovarianAs well as other factors, directly affect how strong surgery will be applied, and whether there is a need to carry out a preoperative (neoadjuvant) and postoperative (adjuvant) chemotherapy.
Surgical treatment of ovarian cancer
Surgical treatment of ovarian cancer It is directed to the maximum amount to remove both the primary tumor and its metastases.
In case of disease cancer of the ovarian, preference is given to the extirpation of the uterus and its appendages, as well as resection of the large gland (in other words, the complete removal of the uterus, the uterine pipes and the ovaries on both sides).
The ovarian cancer uses the concept of a cytotentucleus operation, that is, the operation carried out in order to reduce the volume of the tumor.
The cytioneductive operation can be of two types: optimal (with a tumor size of no more than one centimeter) and non-optimal (with a tumor volume more than one centimeter).
Patients who were not in the first stages were carried out the maximum cytioedection, an intermediate cytiratement operation is carried out, in case there is a positive trend or stabilization of the tumor against chemotherapy.
Chemicherapy of cancer of ovarian
The stage of the disease directly affects which of the chemotherapy options will be used to treat ovarian cancer.
Neoadjuvant chemotherapy (preoperative) It is carried out for patients who are in the first stages are not possible to carry out surgical intervention. After chemotherapy gave the desired results, a surgical treatment can be carried out.
Adjuvant chemotherapy (postoperative) It is carried out after the operation of the patient, depending on the stage of the disease. In the early stages, chemotherapy is carried out for patients with high and intermediate risk. This risk is determined by the genius-oncologist who makes the conclusions based on their various characteristics.
Therapeutic chemotherapy is carried out only in cases of the presence of a relapse of the disease or in the case of the initially strong distribution of the disease.
If, after chemotherapy platinum preparations, there is a relapse of the disease, then it is time from the moment of completion of chemotherapy and before recurrence.
If, after the end of chemotherapy, less than six months have passed until the occurrence of relapse occurred, or it arose during treatment, the tumor is recognized as not sensitive to platinum preparations (platinorestation), and the treatment of these drugs is terminated.
Patients who have a platinor-resistant course of the disease are often not cured and the duration of their life is sharply reduced.
If more than six months passes, the tumor is considered sensitive to platinum preparations (platitically sensitive). If a positive result after paying chemotherapy is held sufficiently long, that is, the high probability of re-reaction to the treatment regimen with these drugs.
First of all, if there are no contraindications, combinations of platinum-based preparations are used, such as a paclitaxel dose of 175 mg / m2 with cableplatinomas6 times every three weeks for six treatment courses.
In addition, carboplatin is combined with a docetaxel, hemcitabine, liposomaldeddox.D.
Subsequent observation
Active observation after treatment consists of :
- Anamnese collection;
- Surveys and inspection;
- Blood analysis on the determination of serum concentration Ca 125. It is done every three months for three years and more than four months in the third year. Further this procedure It repeats once every six months during the fourth and fifth years.
| Methods for the treatment of female genital cancer |
| Chemotherapy |
| Evaluation of the cervix - HPV |
| What you need to know about cervical cancer |
| Cervical Cancer Detection |
| Diagnosis of cervical cancer |
| Cervical cancer |
| Treatment of cervical cancer |
| Ovarian cancer |
| Treatment of ovarian cancer |
| Cancer body uterus |
| Causes of body cancer |
| Endometrial cancer flow |
| Symptoms of body cancer |
| Diagnosis of uterine cancer |
| Methods of treating disease |
| Chemotherapy with uterine cancer |
| Metastasation of uterine cancer |
| Life after the treatment of uterine cancer |
| Forecast when detecting uterine cancer |
| Nepphelial tumors of ovarian |
| Diagnosis of non-epithelial ovarian tumors |
| Treatment of ovarian tumors |