Hoble and osteoporosis study design 14.01 04. Chronic obstructive pulmonary disease and osteoporosis. The Role of Glucocorticoids in the Development of OA in Patients with Hoblas
The relevance of research.
Chronic obstructive pulmonary disease (COPD) is a disease characterized by persistent and progressive airflow restriction associated with chronic inflammation of the airways and lungs by harmful particles or gases, especially from inhaled cigarette smoke. COPD is now recognized as a systemic disease with various comorbidities, including lung cancer, atherosclerosis, osteoporosis, diabetes, anxiety / depression. Management of these comorbidities is clinically important as they are associated with hospital admissions, mortality, and reduced quality of life in patients with COPD. Osteoporosis is one of the main comorbid pathologies in COPD. Although the pathophysiological link between COPD and osteoporosis remains unclear, recent epidemiological studies have clearly shown that osteoporosis is very common in patients with COPD.
Purpose of the study
To assess the prevalence and course of osteoporosis in patients with COPD. Research methods
We studied 75 patients with COPD. Research results
Osteoporosis is a skeletal disorder characterized by impaired bone strength, predisposing a person to an increased risk of fractures. The most important outcome is fracture and the risk of fracture depends on the strength of the bone, which is determined by bone mineral density (BMD) and its quality. According to a systematic review, analyzing only 75 patients with COPD, the prevalence of osteoporosis is determined by a low BMD and was 35.1%. The prevalence of fractures on radiographs in patients with COPD is 24% to 79%, but the values may vary depending on characteristics such as age. , gender and severity of COPD. Data on the quality of bone tissue in COPD are limited: there are almost no data on the material properties of bones, such as degeneration of the bone matrix, the degree of calcification. Bone biopsy is the best way to directly assess the microarchitecture of bone tissue at the tissue level. There is only one report in which histomorphometric analysis was performed on bone biopsies from postmenopausal women with COPD who did not take systemic glucocorticoids. Women with COPD showed significantly low trabecular bone volume and junction density, and decreased cortical width and increased cortical porosity, compared to age-matched postmortem controls. Bond density was negatively correlated with smoking (pack-years), suggesting that structural damage affects bone strength in COPD patients. With regard to bone metabolism in COPD, it should be noted that bone undergoes continuous modernization, and the balance between resorption and formation is critical for maintaining bone mass and quality. Biochemical bone markers are useful for the non-invasive assessment of bone metabolism. It should be noted that there are several factors that can either enhance or suppress bone metabolism to varying degrees in patients with COPD, including vitamin D deficiency, glucocorticoids, immobilization, hypoxia, and so on. Little is known about the mechanisms that lead to osteoporosis in COPD patients. but clinical researches showed that osteoporosis and other systemic comorbidities of COPD are associated with various general and disease-specific risk factors such as systemic inflammation, pulmonary dysfunction, glucocorticoid use and vitamin D deficiency / deficiency. Elderly age and smoking are common risk factors for osteoporosis and COPD. Smoking is an established risk factor for osteoporotic fractures. Weight loss is common in COPD, especially in the advanced stages, and is associated with a poor prognosis. Overall, Body Mass Index (BMI) is a factor in BMD and the risk of fractures in the general population, weight loss and cachexia in severe COPD has been attributed to systemic inflammation with increased levels of cytokines such as tumor necrosis factor alpha (TNF-α) and oxidative stress. which can cause metabolic disturbances in bone tissue directly or indirectly through sarcopenia, the extent to which they contribute to the correlation between BMD and BMI in patients with COPD requires further study.
Disease-specific risk factors for osteoporosis in COPD:
Systemic inflammation. The pathophysiological process of COPD is characterized by infiltration of the mucosa, submucosa and glandular tissue of inflammatory cells in the airways, which leads to an increase in mucus content, epithelial hyperplasia and, as a result, to thickening of the wall respiratory tract.
Chronic inflammation and imbalance between proteases and their inhibitors leads to narrowing, obliteration and destruction of terminal bronchioles. Smoke-induced damage to epithelial cells stimulates the release of early cytokines such as IL-1, interleukin-2 and TNF-α. "Systemic inflammation is reflected elevated level c-reactive protein (CRP), which has been associated with osteoporosis and increased bone resorption, as well as the role of inflammation in COPD-associated osteoporosis. COPD patients with lower BMD showed high levels of CRP and proinflammatory cytokines such as TNF-α, IL-1 and IL-6; COPD-associated osteoporosis. Our preliminary results indicate that systemic inflammation in COPD is associated with disruption of bone microarchitecture. The exact roles of systemic inflammation in COPD, associated osteoporosis and its contribution to fracture risk remain to be determined.
Pulmonary dysfunction. The relationship between lung function and fractures must be interpreted with caution as they can mutually influence each other. Visual effects can cause back pain, deformities chest, kyphosis and decreased growth, all leading to impaired lung function. A systematic review of the relationship between lung function and visual effects in COPD demonstrated that each impairment was associated with a 9% decrease in lung capacity (vl). This study confirmed the presence of a fracture with a decrease in fluid and a fracture in the number with a decrease in FEV1.
Glucocorticoid drugs are a secondary cause of osteoporosis. Glucocorticoid-induced osteoporosis (GIO) is dose dependent but occurs even in low doses. Most recent studies of COPD-associated osteoporosis, however, have included only a small number of subjects taking systemic glucocorticoids, or have shown an increased incidence of fractures in subjects without systemic glucocorticoids.
Vitamin D deficiency / deficiency leads to decreased intestinal calcium absorption, impaired skeletal calcification, and secondary hyperparathyroidism with high bone metabolism, thereby leading to bone loss and an increased risk of fracture. Several studies have shown that vitamin D status does correlate with BMD in COPD subjects, and one study found that in 100 stable COPD patients at baseline, vitamin D deficiency increased the risk of osteoporosis by 7.5 times over a 3-year follow-up period. These results confirm the role of vitamin D deficiency / deficiency in COPD-associated osteoporosis, and its contribution to fracture risk in COPD patients should be more accurately assessed in a large prospective study in the future.
Conclusion. There is ample evidence that osteoporosis and osteoporotic fractures are very common in COPD patients. Although the mechanisms by which COPD leads to osteoporosis is not yet clear, patients with COPD share many common and more specific risk factors for osteoporosis. It is important for pulmonologists as well as general practitioners to be aware of the high prevalence of osteoporosis in COPD patients and to assess their fracture risk. Osteoporosis screening will allow doctors to diagnose COPD patients with comorbid conditions for early stage and provide appropriate treatment to prevent damage that can lead to improved quality of life as well as a longer-term favorable prognosis in these patients.
Bibliography
1. Sudakov O.V. Analysis of the incidence of fractures of various localization in patients with chronic obstructive pulmonary disease on the background complex treatment/ O.V. Sudakov, E.A. Fursova, E.V. Minakov // System analysis and control in biomedical systems. 2011. T. 10. No. 1. S. 139-142.
2. OV Sudakov An integrated approach to the treatment of chronic obstructive pulmonary disease / O.V. Sudakov, E.V. Minakov, E.A. Fursova // GOUVPO "Voronezh State Technical University". Voronezh, 2010.-195 p.
3. Sudakov O.V. An integrated approach to the assessment of individual pharmacotherapy in patients with chronic obstructive pulmonary disease and arterial hypertension / O.V. Sudakov, A.V. Sviridov. -Voronezh: VGTU, 2007. -188 p.
4. Sudakov O.V. The problem of osteoporosis in patients with bronchial asthma and chronic obstructive pulmonary disease during treatment with glucocorticosteroids / O.V. Sudakov // System analysis and control in biomedical systems. 2007. T. 6. No. 4. S. 996-1000.
Back to number
Osteoporosis and chronic obstructive pulmonary disease
Authors: A.V. GLUKHOV, N.E. MONOGAROVA, N.S. KABANETS, T.V. A. T. A. Kugaevskaya LE, I.Yu. CHIBISOVA, Donetsk National Medical University. M.M. Gorky, Department of Internal Medicine. prof. AND I. Gubergrits, Donetsk Regional Clinical Territorial Medical Association (Pulmonary Department)
Summary
The peculiarities of the management of patients with chronic obstructive pulmonary disease (COPD) are determined by various extrapulmonary pathologies of these patients. The interpretation of the existing extrapulmonary pathology is not always unambiguous from the point of view of its pathogenetic relationship with COPD, since many patients (especially senile ones) are characterized by a combination of diseases. This article examines one of the important modern medical and social problems of osteoporosis (OP) in the light of the combination of this disease with COPD.
Chronic obstructive pulmonary disease is a preventable and treatable disease characterized by a restriction of airflow through the airways that is not completely reversible. Airway obstruction, as a rule, progresses and is associated with a pathological inflammatory response of the lungs to the effects of harmful particles or gases, especially tobacco smoking (order No. 128 of the Ministry of Health of Ukraine).
According to the Global initiative for chronic obstructive lung disease (GOLD), COPD is a disease characterized by a combination of clinical manifestations of chronic obstructive bronchitis and emphysema, the proportion of which can be different.
According to the European Respiratory Society, only 25% of patients are diagnosed with the disease in a timely manner. Underdiagnosis of COPD is associated with the fact that patients seek medical help only when severe symptoms appear or even a serious threat to life. At the same time, COPD is in 6th place among the leading causes of death in the world, in 5th place in the developed countries of Europe. COPD is an extremely costly pathology and a significant social burden.
According to WHO forecasts, by 2020, COPD will take the 3rd place in the world in the structure of mortality.
COPD is characterized by systemic disorders that are an important part of a vicious cycle and must always be considered in the clinical management of patients. These include cachexia with loss of fat mass, loss of skeletal muscle and its weakness, osteoporosis, depression, anemia, increased risk of developing cardiovascular disease... Osteoporosis deserves special attention, both as a consequence of the use of corticosteroids and independently developed during the pathogenesis of COPD.
Basic principles of therapy for patients with COPD:
- a gradual increase in the intensity of treatment, depending on the severity of the course of the disease;
- regularity, constancy of basic therapy in accordance with the severity of the course of the disease;
- the variability of the individual response to treatment determines the need for careful and regular monitoring of the clinical and functional signs of the disease.
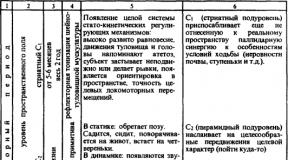
From table. 1 it follows that in the treatment of patients with COPD, starting with Stage III diseases, there is the use of glucocorticosteroids (GCS), which, in turn, can contribute to the development of osteoporosis.
Osteoporosis is a systemic disease of the skeleton, characterized by a decrease in bone mass and a violation of the microarchitectonics of bone tissue, leading to an increase in bone fragility and the risk of fractures.
The most common sites of osteoporotic fractures are the vertebrae, ribs, wrists, femoral neck, and proximal humerus, pelvic bones. Bone fractures often lead to disability and death, which determines the clinical significance of osteoporosis.
Low bone mineral density (BMD) is the main quantitative symptom of osteoporosis. In 1994, a working group of the World Health Organization decided to diagnose osteoporosis based on the degree of BMD reduction, as determined by bone densitometry. In this case, a single universal diagnostic indicator is used for all densitometry methods - the so-called T-criterion, which is defined as the ratio of the actual bone mass of the subject to the peak bone mass of young healthy people of the same sex, calculated as a percentage and standard deviations.
Epidemiology
If we take into account the epidemiological data on the incidence of OP and COPD, then there is an obvious trend towards an increase in the incidence with age. Therefore, it would seem, we can talk about the natural "age-related comorbidity" of COPD and OP. This factor is not in doubt, however, the studies available on this problem indicate that a number of other reasons may be important in the development of AP in patients with COPD, some of which are beyond doubt, while others require clarification. Apparently, one of the first works devoted to the study of the possible connection of AP with chronic pulmonary diseases was a study in patients chronic bronchitis bone mineral density, which was lower compared to the age-matched control group. In later studies, a high incidence of osteopenia and OP in patients with COPD was established, reaching 60%, and as COPD progressed, osteoporosis was detected more often. A high incidence of AP has been established in patients with the terminal stage of various chronic pulmonary diseases (including COPD) who are candidates for lung transplantation. BMD of the spine and hip in comparable age groups was reduced both before and after transplantation.
Clinical manifestations of osteoporosis
Often clinical symptom osteoporosis is pain in the back, in the lumbosacral or sacral region. The feeling of fatigue, the need for frequent rest in the supine position, a fracture of the radius in a typical place and kyphotic deformity, which appear long before the pain, are most often not perceived by patients as symptoms of the disease. The severity of the pain syndrome can be different not only in different patients, but also in the same patient at different intervals. A feature of pain in osteoporosis is that long-term use of non-steroidal anti-inflammatory drugs does not stop it.
Pain is not always associated with fractures, more often its cause is trabecular microfractures. Although the pain in osteoporosis is less intense than in osteomalacia, in some cases it is the pain that confers patients to bed. In the course of the disease, a typical change in the appearance of patients occurs. There is a pronounced thoracic kyphosis, a shortened compressed torso, the ribs reach the crests of the iliac bones. Due to the shortening of the trunk, the skin of the abdomen forms multiple folds. Lumbar lordosis can be excessive or flattened. In most of these cases, there is a pronounced defensive posture with limited mobility. In the English-language literature, this condition is called dowager's hump (widow's hump).
A common symptom in patients with osteoporosis, regardless of its form, is a decrease in growth. Movement in lumbar the spine is limited. Gait disorder is detected not only in patients with fractures of the pelvic bones and femoral neck. A shuffling, unsteady gait with widely spaced feet is often observed in patients with postmenopausal and steroidal forms of osteoporosis and occurs without skeletal fractures.
A long course of the disease without clinical manifestations is possible, up to the occurrence of asymptomatic fractures of the vertebral bodies. Regardless of the number and number of compression fractures of the vertebral bodies in osteoporosis, paresis and paralysis are not observed. In some cases, this is what allows the differential diagnosis of osteoporosis with metastatic lesions of the vertebral bodies.
Instrumental diagnosis of osteoporosis
Standard radiography is the most widely used method until recently for diagnosing both osteoporosis itself and its complications. However, the diagnostic value of radiography depends on a number of factors that are difficult to account for, including the experience of the radiologist.
To objectify the degree of bone mineralization disorders, the so-called semi-quantitative methods have been developed. They are based on the calculation of vertebral, femoral and metacarpal indices. For tubular bones, this is the ratio of the width of the cortical layer to the diameter of the bone; for vertebrae, it is the degree of their deformation, which is often caused by compression fractures.
X-ray changes characteristic of osteoporosis appear when bones lose 20–40% calcium. Moreover, in many cases, the severity of osteopenia on radiographs does not correlate with spinal fractures.
Densitometry - a quantitative study of bone mineral density - is currently one of the most significant methods in the diagnosis of metabolic diseases of the skeleton and almost the only method of non-invasive risk assessment bone injury with osteoporosis. The most widely used are X-ray and ultrasound densitometry, as well as quantitative computed tomography (CKT). With ultrasound densitometry, only some parts of the peripheral skeleton are available for measurement; this technique is more often used for screening.
CKT has sufficient accuracy in examining the spine; its main advantage over other methods is the ability to selectively analyze cancellous and compact bones in terms of bulk density. The main disadvantages of CCT: difficulties in examining the bones of the peripheral skeleton, unacceptably high total radiation exposure during long-term follow-up, and high cost of the study.
Currently, dual energy X-ray densitometry (DXA) is preferred because it is less expensive, more accurate, and produces less radiation. Dynamic observation is determined by the accuracy of the test. The DXA margin of error is 1-3%. This method is currently regarded as the gold standard for bone densitometry. Simultaneously, at least two critical areas of the skeleton are examined (in a typical case, the proximal femur and the spine in frontal projection), which avoids many mistakes, for example, when obtaining overestimated results in one area.
The main factors in the development of osteoporosis in COPD (Fig. 1, 2):
- a chronic inflammatory process, an increase in the production of pro-inflammatory cytokines;
- hypoxia (bronchial obstruction, hypoventilation, decrease in minute volume of respiration, circulatory failure), accumulation of CO2, lactic acid in the blood, chronic respiratory acidosis;
- the use of glucocorticoids;
- immobilization.


Although pulmonologists associate the problem of osteoporosis mainly with taking GCS, research results show that patients who do not take GCS also have a significant risk of developing osteoporosis. In 90% of severe patients, bone tissue hyperresorption is observed. Its occurrence in 40% of cases is associated with a deficiency of vitamin D, in 10% - with bone resorption due to immobilization, in 45% there is a combination of these two factors. Shown, that immobilization even at the 6-8th week. leads to an irreversible loss of 10% of bone density. This decrease in bone density approximately doubles the risk of fractures.
Chronic inflammatory process promotes the formation of a large number of cytokines involved in bone resorption. Normally, they are not detected in the blood, but with severe inflammation, their concentration increases significantly. Early response cytokines (tumor necrosis factor (TNF), interleukins - IL-1 and IL-6) are produced in large quantities when bronchial asthma(BA), pneumonia, tuberculosis, cystic fibrosis, sarcoidosis. They are also involved in the process of bone resorption.
The most compelling evidence comes from TNF, which promotes the proliferation and maturation of osteoclast precursors. IL-1 and IL-6 are also powerful mediators of osteo-clastogenesis (IL-1 is 4-10 times stronger factor of bone resorption in vitro than parathyroid hormone - PG). These and other cytokines provide a link between inflammatory process in the bronchopulmonary system and bone remodeling, which ultimately leads to bone loss.
Important factors are hypoxia, decreased physical activity due to respiratory symptoms and frequent hospitalizations in critically ill patients. It is a known fact that patients with severe pulmonary diseases (BA, COPD, sarcoidosis, alveolitis, cystic fibrosis, after lung transplantation) have low bone density and, as a result, suffer from fractures.
The most common secondary osteoporosis is steroid.
Steroid osteoporosis develops as a result of exposure to bone tissue of an excessive amount of glucocorticosteroids. Osteoporosis during treatment with glucocorticosteroid drugs is due to biological effects natural hormones - glucocortico-steroids, which are based on molecular mechanisms of interaction with glucocorticosteroid receptors of osteoclasts (OC) and osteoblasts (OB). During the first weeks of treatment with GCS, there is a decrease in the absorption of calcium in the intestine. GCS increase renal excretion and decrease tubular reabsorption of phosphorus and calcium. Taking 40 mg of prednisolone for 5 days leads to a 2-fold increase in urinary calcium excretion. There are reports of the direct effect of GCS on the state of receptors and the activity of OB and OK. GCS inhibit the production of PG E2, which stimulate the synthesis of collagen and non-collagen proteins by bone cells. In addition, corticosteroids reduce the amount of sex hormones that have anabolic effects, which can also contribute to osteoporosis. Thus, corticosteroids have a multifaceted effect on bone tissue, which in total activates bone remodeling. The latter leads to an increase in the rate of resorption without compensatory growth of bone formation and, as a result, to the development of osteoporosis.
For steroid osteoporosis trabecular bones are affected axial skeleton- the bodies of the vertebrae, pelvic bones, ribs, femoral neck. For steroid damage to the skeleton in childhood a delay in linear growth is typical. Taking high doses of corticosteroids causes a fairly rapid and significant loss of bone mass. Already in the first 6-12 months. treatment, its loss in 5-15% can be observed. Much loss occurs in the lumbar spine. According to the literature, with equal doses of corticosteroids and the duration of therapy, the development of osteoporosis, like other complications of corticosteroid therapy, has large individual characteristics. This is primarily due to genetic factors that determine the characteristics of GCS metabolism and the state of vitamin D receptors.
There was a high incidence of vertebral compression fractures in elderly men with chronic pulmonary disease(senile osteoporosis), but severe clinical manifestations fractures are most common in those taking glucocorticoids.
The use of inhaled steroids in comparison with parenteral forms leads to a decrease in adverse effects on the skeleton, but does not completely prevent them. Therefore, CT density should be measured in all patients with chronic lung disease. Certain prophylactic regimens should be established for those patients who have low baseline BMD values or are receiving glucocorticoid treatment.
The main clinical manifestations of OP- This is pain and fractures, although bone loss may be asymptomatic and the first sign of OP is bone fractures. Fractures negatively affect the quality of life of patients in general, especially in patients with COPD. Typical localization of fractures in patients with AP is the spine and proximal femur. The clinical significance of vertebral fractures in patients with COPD is a deterioration in the functional capacity of the lungs due to the presence of pain syndrome, as well as progressive kyphosis of the thoracic spine with subsequent restrictive breathing disorders. Thus, in a study of 9 nonsmoking patients with severe kyphoscoliosis, the forced vital capacity (FVC) was 29%, and the total lung capacity was 44% of the due one, while the ratio of forced air volume per 1 s / FVC was within the normal range. According to a study of 74 women with OP, each fracture of the thoracic vertebra reduces FVC by approximately 9%. Spinal deformities resulting from osteoporotic fractures of the vertebrae have a negative effect on the function of external respiration. With vertebral kyphosis in women with OP, the indicators of VC, total lung capacity, inspiratory capacity of the lungs, as well as lateral and vertical mobility of the ribs, are significantly reduced in comparison with healthy women of the same age. At the same time, a negative correlation was noted between the angle of kyphosis and the studied indicators of the function of external respiration (FVD). It should be emphasized that if in individuals with normal pulmonary function the detected changes in pulmonary volumes are not significant, then in patients with COPD, even minimal deterioration in FVD can aggravate functional disorders, worsening the quality of life of patients. In addition, there is evidence that vertebral fractures increase the risk of death in patients with COPD. The clinical significance of vertebral fractures in these patients was the increased risk of exacerbations of COPD, the development of pneumonia in them, which often had a fatal outcome. The most serious consequence of AP is hip fractures, the risk of which increases as BMD decreases and in the presence of concomitant chronic diseases. The occurrence of hip fractures leads to hypomobility, which aggravates functional disorders in patients with COPD, makes patients more dependent on their caregivers, and increases the mortality rate of patients, especially the elderly and senile. These data indicate that AP with subsequent fractures of the spine and other bones is a serious problem in elderly patients with COPD and requires early detection in order to timely correct and prevent the progression of BMD decline. In fig. 3 shows the main consequences and clinical significance of OP in patients with COPD. Currently, the gold standard for the diagnosis of OP or osteopenia is dual-energy X-ray absorptiometry. However, due to its high cost and relatively low availability, the detection of AP and the appointment of appropriate treatment in many patients, including patients with COPD, are belated. Attempts to use the methods of ultrasound densitometry of the calcaneus for the purpose of early diagnosis of AP in patients with COPD, even with the additional use of a special questionnaire, did not materialize. This method turned out to be less sensitive than DXA in the diagnosis of OP and osteopenia in patients various diseases lungs. The authors emphasize that ultrasound evaluation cannot be used as a screening for low BMD values. Bone metabolism is assessed using some markers - serum C-telopeptide and N-telopeptide, bone-specific alkaline phosphatase activity. Recently, the concept of bone quality and criteria for assessing the effectiveness of anti-osteoporotic drugs have been discussed from the standpoint of the modern understanding of the mechanisms of bone fractures in OP. Since it has now been proven that there is no parallelism between an increase in BMD and a decrease in the frequency of fractures, there is reason to believe that some drugs reduce the risk of fractures to a greater extent due to their effect on bone quality than on BMD. Bone quality is assessed using ultrasound examination, magnetic resonance imaging, peripheral computed tomography, bone biopsy.

Treatment and prevention of AP in patients with COPD
Control of extrapulmonary pathology in patients with COPD is an essential component of the management of this category of patients. With regard to OP, this position of the attending physician is of particular importance given the risk of fractures of the spine and hip neck, which significantly impair not only lung function, but also the quality of life of these patients. The management of patients with COPD in combination with OP includes:
- COPD control in the phase of exacerbations and remissions (bronchodilators, mucolytics, antibiotics, glucocorticoids, vaccines, rehabilitation, kinesitherapy, educational programs and etc.);
- control of concomitant pathology;
- physical activity;
- fight against nutritional deficiency;
- the appointment of anti-osteoporotic drugs.
Studies on the use of anti-osteoporotic drugs in patients with COPD concern mainly patients receiving glucocorticoids, which are a proven risk factor for AP.
Vitamin D and calcium supplements
The data obtained on the presence of vitamin D deficiency in patients with COPD are the basis for prescribing vitamin D to these patients. Active metabolites of vitamin D (alfacalcidol and calcitriol), which normalize the absorption and balance of calcium, reduce the secretion of PTH along with the stimulation of bone formation, are of particular importance. In patients receiving systemic GC, it is advisable to prescribe calcium preparations (1000-1500 mg of elemental calcium per day), taking into account a decrease in intestinal absorption of calcium and an increase in its excretion in the urine. In a series of randomized studies, the effectiveness of the combined use of vitamin D and calcium preparations for the prevention of AP in patients taking systemic GC for a long time has been shown. At the same time, it is recommended to control the level of calcium in the blood and urine.
Hormone replacement therapy
Testosterone deficiency in men with COPD, aggravated by treatment with systemic GCs, is one of the factors in the development of AP in this category of patients. Taking into account the decrease in muscle mass in patients with COPD and the catabolic effect of HA, testosterone administration may also have additional indications to increase muscle mass and reduce adipose tissue. The appointment of hormone replacement therapy (HRT) for postmenopausal women who received systemic GC for COPD during the year contributed to an increase in the BMD of the lumbar vertebrae by 4.1%, while in the group of patients who did not receive HRT, there was a further decrease in BMD by 3.4%.
Calcitonin
There are currently no data on the effect of calcitonin on the incidence of fractures in GC-treated patients with COPD. An important property of calcitonin is its pronounced and persistent analgesic effect, which gives the drug additional benefits in patients with AP with pain syndrome. Elimination of pain in osteoporotic fractures in patients with COPD allows avoiding complications caused by pain (prolonged immobilization, hypoventilation, impaired excitation), additional prescription of analgesic drugs, including NSAIDs, to which some patients may be hypersensitive.
Clinical guidelines on the management of patients with COPD with the presence of OP or risk factors for OP:
- control of COPD, respiratory failure, rehabilitation programs;
- encouraging the physical activity of patients;
- correction of nutritional deficiency;
- BMD assessment in patients with COPD with additional risk factors (low body weight, severe respiratory failure, history of fractures, etc.);
- BMD assessment before prescribing GC;
- assessment of BMD in patients with COPD receiving systemic (every 6-12 months) and inhaled (12-24 months) GC;
- the appointment of vitamin D (400-800 IU / day) and calcium preparations (1000-1500 mg / day) for patients with COPD with the presence of risk factors for AP;
- hormone replacement therapy in menopausal women and in men with hypogonadism;
- the appointment of calcitonin or bisphosphonates to patients with COPD with verified OP or risk factors with the ineffectiveness of hormone replacement therapy;
- dynamic assessment of BMD against the background of anti-osteoporotic therapy.
Bibliography
1. Global initiative for chronic obstructive lung disease - GOLD, 2007.
2. Snow V., Lascher S., and Mottur-Pilson C., for the Joint Expert Panel on Chronic Obstructive Pulmonary Disease of the American College of Chest Physicians and the American College of Physicians - American Society of Internal Medicine. Evidence base for management of acute exacerbations of chronic obstructive pulmonary disease // Ann. Intern. Med. - 2001. - Vol. 134. - P. 595-9.
3. Franke Y., Runge G. Osteoporosis. - M .: Medicine, 1995 .-- S. 12-15.
4. Benevolenskaya L.I. Osteoporosis - actual problem medicine // Osteoporosis and osteopathy. - 1998 .-- S. 4-7.
5. Povoroznyuk V.V. Osteoporosis: clinic, diagnosis, prevention, treatment // Zhurn. practical doctor. - 1996. - No. 6. - S. 18-35.
6. Deckweiker J. Strategy for the treatment of osteoporosis // First Russian symposium on osteoporosis. - M., 1995 .-- S. 21-28.
7. Delmas P.D. Mechanisms of bone loss in osteoporosis // Abstracts of lectures and reports of the 1st Russian symposium on osteoporosis. - M., 1995 .-- S. 31-33.
8. Nasonov E.L. Secondary osteoporosis: pathogenesis and clinical significance in inflammatory diseases of the joints // Osteoporosis and osteopathy. - 1998. - No. 1. - S. 18-22.
9. Smith R. Investigation of osteoporosis // Clin. Endocr. - 1996. - Vol. 44 (4). - P. 361-374.
10. Leparskiy E.A., Skripnikova I.A. Diagnosis and treatment of osteoporosis ( state of the art question). - M., 1997 .-- S. 26.
11. Praet J. P., Peretz A., Rosenberg S. et al. Risk osteoporosis in men with chronic bronchitis // Osteoporos Int. - 1992. - Vol. 2. - P. 257-261.
12. Iqbal F., Michaelson J., Thaler L. et al. Declining bone mass in men with chronic pulmonary disease. Contribution of glucocrticoud treatment, body mass index, and gonadalfunction // Chest. - 1999. - Vol. 116. - P. 1616-1624.
13. Incalzi R. A., Caradonna P., Ra-nieri P. et al. Correlates of osteoporosis in chronic obstructive pulmonary disease // Respir. Med. - 2000. - Vol. 94. - P. 1079-1084.
14. McEvoy C. O., Ensrud K. E., Bender E. et al. Association between corticosteroid use and vertebral fractures in older men with chronic obstructive pulmonary disease // Am. J. Respir. Crit. Care Med. - 1998. - Vol. 157. - P. 704-709.
15. Del Pino-Montes J., Fernan-des J. L., Gomez F. et al. Bone mineral density is related to emphysema and lung function in chronic obstructive pulmonary disease // J. Bone Miner. Res. - 1999. - Vol. 14 (suppl.). - SU 331.
16. Snow V., Lascher S., Mottur-Pilson K. Clinical guidelines. Part I. / Substantiation of management tactics for patients with exacerbations of chronic obstructive pulmonary diseases. // International Journal of Medical Practice.
17. Chuchalin A.G. Chronic obstructive pulmonary disease and concomitant diseases // Health of Ukraine. - 2008. - No. 15-16. - S. 37-39.
NAUMOV
ANTON VYACHESLAVOVICH
Prevalence and course of osteoporosis in patients with somatic diseases
Moscow - 2010
The work was done in the State educational institution higher professional education "Moscow State University of Medicine and Dentistry"
Scientific consultant:
Honored Scientist of the Russian Federation,
Doctor of Medical Sciences, Professor Arkady Lvovich Vertkin;
^ Official opponents:
Academician of RAMS, professor Martynov Anatoly Ivanovich
Doctor of Medical Sciences, Professor Stryuk Raisa Ivanovna
Doctor of Medical Sciences, Professor Alekseeva Lyudmila Ivanovna
Lead organization:Russian state medical University them. N.I. Pirogov
The defense will take place "___" ______________ 2010 at ___ hours at a meeting of the Dissertation Council D.208.041.01. at the State Educational Institution of Higher Professional Education "Moscow State University of Medicine and Dentistry of Roszdrav" (127473, Moscow, Delegatskaya st., 20/1)
The thesis can be found in the library of the State Educational Institution of Higher Professional Education MGMSU of the Federal Health Service (127206, Moscow, Vuchetich St., 10a)
The abstract was sent "____" ______________ 2010
Scientific Secretary of the Dissertation Council
Doctor of Medical Sciences, Professor Yushchuk E.N.
^ RELEVANCE OF THE PROBLEM.
According to official statistics, an average of 105.9 cases of fractures are diagnosed annually in the Russian Federation in people over 50 years old. proximal femur per 100,000 population (78.8 and 122.5 for men and women, respectively). The leading cause of such fractures is osteoporosis, a progressive systemic skeletal disease characterized by a decrease in bone mass and a violation of the microarchitectonics of bone tissue, leading to an increase in bone fragility and the risk of fractures (WHO, 1999).
According to the report of the International Osteoporosis Foundation (IOF, 2006), after 50 years of complications of this disease, every third woman and every fifth man are diagnosed with this disease, and a third of them die within the first year after an osteoporetic hip fracture. It is for this reason that osteoporosis takes the 4th place in the structure of mortality among the world's population after cardiovascular pathology, diabetes mellitus (DM) and oncological diseases, which indicates the high medical and social significance of the problem (Johnell O. et all, 2004).
At the same time, in the modern literature, when discussing osteoporosis issues, more attention is paid to postmenopausal women, during which excessive activation of bone resorption, induced by estrogen deficiency, leads to a significant loss of bone mineral density (BMD). However, according to E.L. (2005) in 20% of cases the disease occurs in men. Moreover, one third of all cases of osteoporetic hip fractures in the world occur in males, and their immediate and long-term consequences are more severe than in women. Thus, inpatient and outpatient (within a year) mortality after hip fractures in men is 2 times higher than in women (Terrence H. et al., 1997), averaging 40% and 20%, respectively. In addition, about half of men with osteoporosis who have had hip fractures are more disabled and require daily help from medical and social workers. This position is of paramount importance for Russia, where the incidence and premature mortality of men is much higher than in other countries.
According to the official data of the Ministry of Health and Social Development of the Russian Federation, published in 2009, the highest mortality rate in the country is mainly determined by cardiovascular diseases (CVD), which account for 56.6%. At the same time, according to autopsy data, stationary mortality from heart and vascular diseases in Moscow is 48.8%, including more than half of acute vascular accidents (Vertkin A.L., 2009). The situation is further complicated by the fact that patients over 50 years of age who have died from cardiovascular pathology have more than three background or concomitant diseases. Interesting in this regard are the data of Dashdamirov A.Kh., (2005) and Goruleva E.I. (2008) showed that more than 60% of patients with CVD have risk factors for osteoporosis, which is consistent with the results of the study by Farhat G. N., et al. (2007), demonstrating lower BMD values in the vertebral bodies, femoral neck and distal forearm in this category of patients. Moreover, according to U. Sennerby et al. (2007) with cardiovascular pathology there is a manifold increase in the risk of fracture of the proximal femur, and according to Vasan R.S., et al. (2003) among similar patients, the majority have a high level of proinflammatory cytokines in combination with osteoporosis. These data allowed Marcovitz P.A. et all (2005) believe that loss of BMD is one of the predictors of CVD development.
It is well known that one of the main underlying diseases in cardiovascular pathology is type 2 diabetes. According to A.L. Vertkin. (2009) among 3239 autopsies of patients who died in a multidisciplinary hospital, 19% had diabetes, including 97, 1% had type 2. About 50 years ago, Albrigt and Reifehstein hypothesized that diabetes may cause a decrease in bone mass. Today this condition is called diabetic osteopenia. It is especially pronounced in men with cardiovascular pathology (Ermachek E.A., 2006). Diabetes mellitus of the second type develops, as a rule, after 30 years, when the age-related decrease in the secretion of total testosterone begins in men, which leads to the onset of androgen deficiency, which, according to Amin S. et all, (2000) and Khaibulina E.T. (2007) is the main cause of osteoporosis. In the study of Dedov I.I. (2005) and Khalvashi R.Z., (2008) it is shown that approximately 2/3 of men with hypogonadism are diagnosed with reduced bone density, including one third - osteoporosis.
The second place in the country in terms of mortality is occupied by oncological diseases (Ministry of Health and Social Development, 2009). At the same time, according to the autopsy data of deceased patients in general somatic departments, malignant neoplasms are diagnosed in 6 - 8% of cases (Vertkin A.L., 2009). Cancer patients (including those already conditionally cured) are also at risk of developing osteoporosis and its complications. There are a number of explanations for this, including the forced intake of cytostatics, hormonal levels changed after surgery, etc. (NP Makarenko, 2000). It is important to emphasize that the earlier the influence of unfavorable factors on the bone is observed, the higher the risk of developing osteoporosis and fractures already at a young age (Mahon S., 1998).
Another reason contributing to the high incidence of osteoporosis and associated fractures is chronic obstructive pulmonary disease (COPD). This pathology is in 13% of cases the cause of death in patients in a general hospital (Vertkin A.L., 2009).
According to epidemiological studies by Van Staa T.P. et al. (2001) conducted for 5 years in patients with COPD, in about half of the cases, either osteopenia or osteoporosis is diagnosed. The authors explain the obtained results primarily by common risk factors for COPD and osteoporosis (smoking, vitamin D and body weight deficiency), long-term intake of glucocorticosteroids, activation of bone resorption under the influence of mediators of systemic inflammation: TNF-α and interleukin-6 (Eid AA, et al. 2005).
Thus, the data presented provide convincing evidence of the role of somatic pathology in patients with osteoporosis. This is of particular relevance in connection with the increase in the number of people over the age of 65 with a high comorbid background. According to experts' forecasts, the costs of these individuals for the treatment of osteoporotic fractures and, above all, of the femoral neck will increase progressively, and by 2025 they will amount to 31.8 billion euros (IOF, 2006).
To prevent a situation so unfavorable for any society, the global strategy is timely diagnosis and prevention of disease in the general population (IOF, 2001-2007), and identification of patients at high risk of developing fractures (Michigan Quality Improvement Consortium; 2008).
In this regard, it is of interest to identify early markers of osteoporosis using simple clinical manipulations (IOF, 2005). Among them are the studies by Mohammad A.R. et al., (2003) demonstrated that patients with missing teeth have low BMD values. This led the authors to assume that tooth loss due to periodontal disease can be considered a marker of systemic loss of BMD. This can be confirmed by the still few clinical studies showing that women with chronic generalized periodontitis have more than 3 times higher risk of osteoporosis than patients without significant lesions of the oral mucosa (Gomes-Filho S. et al. , 2007). Similar data were obtained in the studies of Wactawski-Wende J. et al., (2005), according to which menopausal women had a significantly higher risk of chronic generalized periodontitis with a reduced BMD.
Traditionally, the diagnosis, prevention and treatment of osteoporosis are a priority, first of all, for rheumatologists, less often for endocrinologists and gynecologists. This is due to the fact that most studies on the effectiveness of treatment of osteoporosis with antiresorptive drugs were carried out mainly in the population of postmenopausal women, and the criteria for exclusion were severe somatic diseases (Povoroznyuk V.V., 2003).
At the same time, the Russian health care system provides the primary health care sector with ample opportunities to implement a set of measures for primary and secondary prevention of diseases in most patients (L.I. Benevolenskaya, 2007; I.V. Galkin et al., 2009). Therefore, the transfer of the center of gravity for the early detection of osteoporosis to local polyclinics will significantly improve the provision of medical care with this and highly common pathology. Development of effective screening programs, clinical features, prevention and treatment of osteoporosis in somatic patients and this study is devoted.
^ PURPOSE OF THE STUDY
Determination of the prevalence, clinical and prognostic value of osteoporosis and methods of its optimal drug correction in patients with somatic pathology.
^ RESEARCH OBJECTIVES
Develop a program for the detection, prevention and treatment of osteoporosis based on multidisciplinary medical institutions
To conduct a retrospective analysis of the features of the comorbid background in patients who have undergone atraumatic fracture of the proximal femur.
To carry out a comparative histomorphological analysis of the state of bone tissue in patients with somatic pathology.
To assess the prevalence of osteopenia and osteoporosis in patients with comorbid conditions
Clarify the gender characteristics of bone mineral density loss in patients with somatic diseases.
To study the role of osteoporosis screening in patients with periodontal disease as an early marker of BMD loss
To determine the effectiveness of programs for the prevention and treatment of osteoporosis in patients with somatic diseases.
For the first time, osteoporosis was screened on a large sample of patients with somatic pathology. It was shown that out of 8600 patients with various diseases internal organs in 34.3% of cases osteoporosis is diagnosed, while out of 1200 patients without chronic somatic diseases, it was detected only in 18.6% of cases. At the same time, the loss of BMD is observed in 77.5% of patients with somatic pathology.
It was revealed that OP is more often detected in patients with cardiovascular pathology, COPD, and oncological diseases. Osteopenia is more commonly diagnosed in patients with type 2 diabetes. The severity of BMD loss in any somatic disease significantly exceeds that in the control group.
It was stated that the most significant risk factors for osteoporosis, both in men and women, are hypogonadism in combination with somatic pathology (reliability of the factor p = 0.013 and p = 0.014, respectively).
It has been shown that almost all patients with atraumatic fracture of the proximal femur have chronic somatic diseases, at different times before the fracture, all of them have repeatedly consulted a therapist. Atraumatic fracture of the proximal femur occurs more often in women (the ratio of men to women is 1: 3), mainly in old age (77.3 ± 7.5), but in men, almost 7 years earlier. These patients, in the overwhelming majority of cases, undergo surgical procedures depending on the type of traumatic injury.
A histomorphometric study in the bone tissue of patients who died not from somatic diseases revealed a predominance of the matrix over the number of resorption cavities, while in patients who died from somatic diseases, an inverse relationship was observed, and a significant decrease in newly formed bone units was also noted (Haversseye systems). These ratios remain valid even when adjusted for age. This is evidence of a significant loss of bone mass and density in patients with somatic pathology, in contrast to patients whose death did not occur from somatic diseases.
For the first time, as an early clinical marker of OP, it was proposed to consider the pathology of the periodontal complex. It was determined that in the presence of osteoporosis, periodontal damage is practically independent of the degree of BMD loss, while in patients with osteopenia, and to a greater extent in patients without BMD loss, the severity of periodontal damage is proportional to the BMD level.
The study revealed that the prevention of osteoporosis in patients with somatic pathology (education of patients, lifestyle changes, appointment combination drugs calcium and vitamin D3) leads to an increase in BMD by more than 7% in the first two years. While only education and lifestyle changes are accompanied by additional loss of BMD and the development of OP in almost 15% of patients in the next two years.
The most effective antiresorptive drugs for the treatment of AP in patients with somatic pathology are ibandronic acid, semi-synthetic salmon calcitonin, and alendronic acid. Patients with somatic pathology and OP who do not receive antiresorptive drugs will additionally lose 5.6% of BMD in the next two years (р
^
PRACTICAL SIGNIFICANCE.
For the first time, on the basis of a multidisciplinary hospital, a city office of osteoporosis was created for screening, diagnostics and treatment of osteoporosis in patients with somatic pathology, equipped with a bone densitometer, which allows performing X-ray, two-photon absorptiometry of the distal forearm.
For the first time, “additional” risk factors for AP in patients with somatic diseases have been identified. Thus, inadequate blood pressure control, hypercholesterolemia and organ lesions in CVD (LVH, impaired myocardial contractility) are prognostically less favorable for BMD loss. In patients with COPD, the presence of chronic obstructive bronchitis and the use of systemic steroids are also unfavorable for the course of AP, however, the use of corticosteroids contributes to some preservation of BMD. In patients with type 2 diabetes - age, as well as inadequate control carbohydrate metabolism contribute to additional loss of VO2 max. With oncological pathology, patients who have undergone radical surgery on thyroid gland, mastectomy, as well as with the localization of a malignant formation in the kidney or prostate require special attention of doctors in terms of identifying and correcting osteoporotic changes in bone tissue.
In the structure of somatic pathology of patients who have undergone an atraumatic fracture of the proximal femur, cardiovascular pathology, type 2 diabetes and COPD prevail, their combination is more often (86.3%). This is reflected in the prognosis of the disease, both in the early inpatient and in the long-term periods. So, hospital mortality is 6.2%, and every fourth dies within the first year after the fracture as a result of the development of acute coronary events, thromboembolism pulmonary artery and erosive and ulcerative bleeding from the upper digestive tract.
The study revealed that, despite the slightly higher prevalence of osteoporosis and osteopenia in menopausal women, in the presence of androgen deficiency in men, BMD losses are more significant than in women with hypogonadism.
It was revealed that in patients with osteoporosis, the state of the periodontal complex is characterized by a significantly greater lesion than in patients with osteopenia and without loss of BMD. Computed radiovisiography can serve as a screening tool for detecting low BMD. A moderate, significant correlation was found between the optical density of the alveolar bone and the BMD of the peripheral skeleton, measured by bone densitometry (r = 0.4, p = 0.002).
The study did not reveal a statistically significant difference in the effectiveness of drugs with a combination of calcium and vitamin D3 and with a combination of calcium, vitamin D3 and magnesium for the prevention of AP in patients with somatic pathology. All modern antiresorptive drugs for the treatment of osteoporosis are effective in patients with somatic diseases. Moreover, their appointment in complex therapy leads to better control of the main symptoms of somatic pathology.
^ PERSONAL PARTICIPATION OF THE DISSERTANT IN THE DEVELOPMENT OF THE PROBLEM.
The dissertation candidate independently carried out the recruitment of patients, their clinical, instrumental and laboratory examination, filling in the corresponding and specially designed registration forms and clinical cards for this study. The author was directly involved in the creation of the city office of the Moscow Department of Health for the diagnosis and treatment of osteoporosis. The author personally carried out statistical processing of the generalized material, made scientific conclusions and presented practical recommendations.
^ BASIC PROVISIONS FOR PROTECTION.
There is a high prevalence and low detection rate of osteoporosis in patients with somatic pathology.
Somatic pathology is a factor that aggravates the loss of bone mineral density.
Periodontal disease may serve as early markers of osteoporosis.
The inclusion of anti-osteoporotic therapy in complex therapy somatic diseases, leads to an increase in bone mineral density and increases the effectiveness of treatment of the underlying disease.
The results of the work are introduced and used in the practice of the city office for the diagnosis and treatment of osteoporosis of the Moscow Department of Health (DZ) on the basis of the outpatient department of the City Clinical Hospital No. 81, polyclinics No. 81 and No. clinical hospital(GKB) DZ of the city of Moscow, cardiological, therapeutic and endocrinological departments of GKB No. 20, No. 50 and No. 81 of DZ Moscow, and in educational and methodological work with students and cadets of the faculty of postgraduate education at the department clinical pharmacology, pharmacotherapy and emergency medical care MGMSU.
^ APPROBATION OF THE DISSERTATION
The dissertation materials were reported at the Siberian National Congress "Human Health as the Basis of National Security" (Krasnoyarsk, 2006), the International Scientific and Practical Conference "Osteoporosis: Epidemiology, Clinic, Diagnostics, Prevention and Treatment" (Evpatoria, Ukraine, 2006), the All-Russian Congress on Andrology (Sochi, 2007), 1st European Congress of the Aging Male (Warsaw, Poland, 2007), II Congress of Cardiologists of the Siberian federal district(Tomsk, 2007), the Joint Russian National Congress of Cardiologists and the Congress of Cardiologists of the CIS countries (Moscow, 2007), the XI Congress of the Russian Society of Urologists (Moscow, 2007), the I and II National Congress of Physicians (Moscow, 2006, 2007), the Round Table “ Men's health as a demographic factor ”of the Committee on Social Policy of the Federal Assembly of the Russian Federation (Moscow, 2007) and at the inter-institutional interdepartmental clinical conference of the staff of the Research Institute of Rheumatology of the Russian Academy of Medical Sciences, the Departments of Clinical Pharmacology, Pharmacotherapy and Emergency Medicine and Dentistry of General Practice and the Training of Dental Technicians of the FPDO MGMSU.
PUBLICATIONS
^ STRUCTURE AND SCOPE OF THE DISSERTATION
The dissertation work is presented on 250 pages of typewritten text and consists of an introduction, a review of literature, materials and research methods, a chapter with research results, conclusions, conclusions, practical recommendations and a list of references. The thesis is illustrated with figures and a table. The literature list includes sources (domestic and foreign).
^ MATERIALS AND METHODS.
The possibility of screening osteoporosis in patients with somatic pathology was implemented on the basis of the city office of osteoporosis of the Moscow Healthcare Department, established in 2004, on the basis of the outpatient department of the City Clinical Hospital No. 81. The office is located on the territory of the X-ray department and is equipped with a DTX 200 bone densitometer (Osteometr, Denmark) and a Lunar DPX BRAVO for X-ray two-photon absorptiometry, medical scales, a height meter, a computer system, audio and video equipment.
A total of 12,985 clinical cases were studied in the study. The study consisted of 6 stages, the design is shown in Figure 1. The criterion for inclusion in the OP screening was: age over 30 years. Exclusion criteria: age less than 30 years, ARVI, presence cancer Gastrointestinal tract, hematological diseases, fever.
Screening was carried out for 5 years, the total number of included patients was 10,200, divided into 2 groups: A and B.
| ^ SCHEME No. 1. RESEARCH DESIGN |
|||||
| Estimation of the prevalence of BMD loss in somatic patients | n = 10 200, Based on the established (2004) city office for the prevention and treatment of osteoporosis |
||||
| ^ Evidence for the relationship between therapeutic pathology and OP | Retrospective study | ABSOLUTELY PROVEN OSTEOPOROSIS - HIP FRACTURE, n = 227 |
|||
| Morphological examination | ^ SOMATIC PATHOLOGY IS ABSOLUTELY PROVEN, |
||||
| Prospective study | Features of the course of osteoporosis and somatic diseases with their combination | CCZ, n = 396 |
|||
| COPD, n = 151 |
|||||
| DM type 2, n = 134 |
|||||
| Oncology, n = 300 |
|||||
| ^ Early clinical markers | Sexual characteristics | Men, n = 721 |
|||
| Women, n = 1111 |
|||||
| Dental diseases | Research, n = 158 |
||||
| Screening, n = 2400 |
|||||
| ^ INFORMATION OF THERAPEUTIC SPECIALISTS ON THE PROBLEM OF OP |
|||||
| EFFICIENCY OF PREVENTION OF OSTEOPOROSIS IN THERAPEUTIC PATIENTS |
|||||
| ^ EFFECTIVENESS OF TREATMENT OF OSTEOPOROSIS IN THERAPEUTIC PATIENTS |
|||||
Group A included 8,600 patients with various therapeutic (somatic) pathologies, the average age of patients was 57.3 ± 6.4 years, including 6255 (72.7%) women and 2345 (27.3%) men ... The structure of somatic pathology is presented in table. 1. It should be noted that these diagnoses were ascertained from the form - referrals for densitometry and the patients were not subjected to a more precise diagnosis.
Group B included 1600 patients, conditionally without somatic pathology. In this group, the average age of patients was 54.3 ± 9.3 years, among them - 1134 (70.9%) - women and 466 (29.1%) - men. In most cases, these were women during the perimenopause period who underwent a routine examination, a number of patients with community-acquired pneumonia, colds, and patients undergoing medical examination.
^
Table 1. The structure of somatic pathology in group A.
| PATHOLOGIES | % of patients | ^ Average age | Floor |
| Cardiovascular diseases (including ischemic heart disease, hypertension and their combinations) | 69 | 57.3 ± 6.4 years | 6255 (72.7%) women 2,345 (27.3%) men |
| ^ Cardiovascular disease and type 2 diabetes | 19,8 |
||
| SD type 2 | 2,2 |
||
| COPD | 1,5 |
||
| ^ COPD plus CVD | 2,7 |
||
| Oncological diseases | 2,9 |
||
| ^ Alcoholic polyvisceropathy | 1,5 |
||
| Rheumatic diseases (RA, SLE) | 0,3 |
We divided the study of evidence of the relationship between therapeutic pathology and osteoporosis into three stages: in the presence of absolute evidence of OP (specific OP complications - fracture of the proximal femur), study the therapeutic history; in the presence of absolute evidence of therapeutic pathology (data from pathological studies), to study the state of bone tissue; within the framework of the study, clarify the therapeutic diagnosis of the patient and identify the relationship clinical picture OP and therapeutic disease.
We studied the medical histories of 227 patients with a femoral fracture at the age of 76.8 ± 7.4 years, including 54 (23.8%) men and 173 (76.2%) women hospitalized in the traumatology department. In all patients, the traumatic force did not exceed the fall from their own height, and the fracture can be classified as domestic. All patients were admitted to the hospital on average 1–3 hours after the injury, and the duration of inpatient follow-up was 23.5 ± 13.8 days. Surgical interventions were performed in 197 (86.8%) patients: skeletal traction, osteosynthesis, hip joint replacement. 17 (7.5%) patients underwent conservative therapy... 58 of 227 patients died, including 14 in the hospital, 44 within a year after discharge. In addition to studying the archival medical history, the discharged patients underwent a telephone survey. In all cases, it was clarified whether osteoporosis was diagnosed before the fracture, if so, what therapy they received, which specialists were observed before the fracture (therapist, gynecologist, endocrinologist, rheumatologist, urologist). In addition, risk factors for osteoporosis were identified in accordance with the international minute test (WHO, 1999).
In the first part of the morphological study, we performed bone densitometry in the corpses of patients who died from somatic pathology. 53 studies were carried out, including 17 in the corpses of men. The average age at the time of death was 72.2 ± 14.5 years. In the structure of the pathological findings, as the main diagnosis, there were: IHD (IHD. Acute myocardial infarction - 17 (32.1%), IHD. Postinfarction cardiosclerosis - 19 (35.8%); Acute cerebrovascular accident by ischemic type - 8 (15.1%); COPD - 9 (16.98%)
In 36 (67.9%) cases, the presence of arterial hypertension, in 14 (26.4%) - diabetes mellitus type 2. In none of the cases on the basis of morphological examination were found rheumatological diseases, and in the clinical and pharmacological history - taking systemic steroids.
For histomorphological analysis of the state of bone tissue in patients with therapeutic pathology, bone tissue samples were preliminarily studied in 14 young individuals (7 men and 7 women) aged 36.6 ± 2.1 years ( morphological control group), who died from automobile traumatic brain injury. V medical documents(accompanying coupons and cards of ambulance calls, medical histories and protocols of forensic medical examination) of all 10 deceased there was no mention of any somatic pathology, risk factors for osteoporosis (age over 65 years, sex hormone deficiency, suffered atraumatic fractures, admission steroids, smoking, alcohol abuse) and clinical and radiological signs of osteoporosis.
V investigated morphological group 30 corpses (14 men and 16 women) aged 69.3 ± 14.3 years were selected, who died from severe somatic pathology, including 12 from ischemic stroke, 13 from myocardial infarction and 5 from alcoholic polyvisceropathy. In all cases, there were risk factors and pathomorphological signs of osteoporosis (thinning and disappearance of trabeculae, an increase in intertrabecular spaces, with filling of the latter connective tissue). A comprehensive morphological study was carried out at the Moscow City Center for Pathological Research. Bone tissue preparations made from the epiphysis of the femur and the iliac crest on the right were examined.
For a prospective analysis of the relationship between OP and therapeutic pathology, we decided to clarify whether the degree of BMD loss depends on the type of pathology and the presence of standardized organ lesions.
Group I included 396 patients, including 342 with hypertension and 54 with coronary artery disease. Among them there were 346 women (87.4%) and 50 men (12.6%) aged 61.6 ± 9.4 years. The study did not include patients with acute forms Ischemic heart disease and cerebrovascular accidents, as well as patients with paroxysmal arrhythmias and chronic heart failure of FC III-IV (according to NYHA). The average duration of cardiovascular pathology in this group was 8.6 ± 4.3 years. Patients with hypertension underwent 24-hour blood pressure monitoring (ABPM) according to the standard method before and after 12 months of treatment. Patients with coronary artery disease underwent Holter ECG monitoring according to the standard technique with continuous recording of three leads for 24 hours. Of 54 patients, 20 (37.1%) had transient ischemic changes, including 17 (85.0%) accompanied by angina pectoris.
^
Table 2. Characteristics of patients with somatic pathology and risk factors for osteoporosis
| Groups / Specifications | Group I (CVD) | Group II (COPD and BA) | Group III (type 2 diabetes) | Group IV (oncologist. pathology) | Group V (control) |
|
| n = | 396 | 151 | 134 | 300 | 194 |
|
| Age | 61.6 ± 9.4 | 60.3 ± 11.2 | 62.3 ± 7.8 | 52.6 ± 12.3 | 58.6 ± 4.3 |
|
| Floor | M | 50 (12,6%) | 21 (13,9%) | 32 (23,9%) | 151 (50,3%) | 40 (20,6%) |
| F | 346 (87,4%) | 130 (86,1%) | 102 (76,1%) | 149 (49,7%) | 154 (79,4%) |
|
| BMI, kg / m2 | 29.2 ± 6.8 | 29.7 ± 5.8 | 30.4 ± 4.6 | 24.3 ± 3.8 | 30.2 ± 4.8 |
|
Osteoporosis in COPD patients: comorbidity or systemic manifestation?
L.I.Dvoretsky, E.M. Chistyakova MMA them. I.M.Sechenov
Epidemiological data indicate an obvious trend towards an increase in the incidence of chronic obstructive pulmonary disease (COPD) and osteoporosis (OP) with aging. Therefore, it would seem, we can talk about the natural "age-related comorbidity" of COPD and OP. However, the studies available on this problem suggest that the development of osteoporosis in patients with COPD may be one of the systemic manifestations of pulmonary disease. According to the GOLD definition (latest revision), COPD is a chronic environmentally mediated inflammatory disease. respiratory system with a predominant lesion of the distal respiratory tract and pulmonary parenchyma with the development of emphysema, manifested by partially reversible bronchial obstruction, progressive respiratory failure and systemic manifestations.
One of these manifestations along with loss of muscle mass, arterial (pulmogenic) hypertension, anemia and depression is OP. The latter is characterized by a decrease in bone mass, impaired bone microarchitectonics and an increased risk of fractures, which determines the medico-social significance of this pathology. There are primary (postmenopausal and senile) and secondary (against the background of various diseases and treatment with certain medications) osteoporosis. Among secondary AP, various lung diseases, including COPD, appear as one of its causes. However, for a wide circle of practitioners, the reality of AP in patients with COPD, its clinical significance, possible mechanisms of formation and management tactics of patients with such a combination remain little known.
Already in the first studies devoted to the study of the possible connection of AP with chronic pulmonary diseases, in particular, chronic bronchitis and COPD, a lower mineral density of bone (BMD) was established in comparison with the control group comparable in age. The incidence of osteopenia and OP in patients with COPD reached 60%, and as the pulmonary pathology progressed, OP was detected more often. The incidence of AP turned out to be especially high in patients with the terminal stage of various chronic pulmonary diseases, including COPD, who are candidates for lung transplantation.
Risk factors for developing AP in patients with COPD
Among the main risk factors for the development of AP in COPD, smoking, low body weight, vitamin D deficiency, hypogonadism, hypomobility, systemic effects, glucocorticoid therapy can be discussed.
Smoking is an independent risk factor for the development of AP in women and men. The BMD in smokers (more than 20 patches) is 12% lower than in non-smokers, and the risk of fractures of the spine and hip in smokers is higher than in non-smokers. Smoking in combination with excessive alcohol consumption increases the risk of developing AP and bone fractures. In smokers and alcohol abusers, the relative risk of vertebral fractures in the 60-69 age group is 3, and among those over 70 it reaches 20.2. A positive correlation was found between the bone formation marker os-theocalcin, BMD and patch-coat index. Thus, smoking is a common risk factor for the development of COPD and AP. However, since almost every patient with COPD smokes, it is difficult to determine the true contribution of smoking and bronchopulmonary pathology itself to the development of OP in this category of patients.
Vitamin D deficiency. It was reported about a significant decrease in the level of 25-hydroxyvitamin D in male patients with COPD who did not receive glucocorticoid therapy, compared with a control group of persons of a similar age. A correlation was found between the level of the inactive form of vitamin D and exposure to sunlight. Moreover, a significant decrease in the level of 25-hydroxyvitamin D was found in 35% of patients with terminal stage COPD before lung transplantation. Many patients with COPD, due to pronounced respiratory failure, are limited in their active movement and practically do not leave the house, and therefore are deprived of sunlight. A similar situation is aggravated in elderly patients with COPD, burdened, in addition, with various diseases (osteoarthritis, stroke, Parkin sonism, heart failure, etc.), causing hypomobility. In such patients, insufficient exposure to sunlight becomes essential in the development of vitamin D deficiency. / l (norm 25-137 nmol / l). At the same time, an inverse relationship was revealed between the level of 25 OHGO and PTH, which may be an additional risk factor for the development of AP.
Weight loss. It is known that BMD indicators are directly correlated with body mass index (BMI). BMD is lower with a lower BMI in both women and men, which, on the one hand, can be explained by a decrease in the load on the bones, and on the other hand, by a higher level of estrogens in overweight individuals due to increased transformation of testosterone into estrogens in adipose tissue. Often, as COPD progresses, weight loss is observed, especially among patients with the so-called emphysematous type of COPD. At one time, even such a term as "pulmonary kakhe-xia" was introduced. Loss of body weight is said in cases where the BMI, which characterizes the ratio of body weight to body surface, is less than 20 kg / m 2. Many hypotheses have been put forward regarding the mechanisms underlying weight loss in COPD, including insufficient food intake, increased energy expenditure, systemic inflammation, tissue hypoxia, and drug therapy. The lowest BMD indices were noted in COPD patients with BMI below the average norm, and a positive correlation was found between BMD and BMI. According to other data, BMI was found to be a predictor of OP in patients with COPD. In patients with COPD with the presence of OP, a lower BMI and adipose tissue were revealed, as well as lower indicators of forced expiratory volume in 1 second (FEV 1) and vital capacity of the lungs (VC) compared with patients in whom the diagnosis - osteopenia was diagnosed.
In our study, we managed to identify high degree correlations between BMI and BMD indicators of the lumbar vertebrae. The correlation coefficient was 0.479 (p = 0.001) for a 1, 0.483 (p = 0) for a 2, 0.479 (p = 0) for a 3, 0.425 (p = 0.004) for a 4, 0.547 (p = 0 ) for the right femoral neck and 0.663 (p = 0) for the left (Fig. 1).
The revealed correlation between BMD (T-criterion and BMD) and BMI may be important in terms of the development of such systemic manifestations of COPD as OP and weight loss.
Hypogonadism. Various chronic diseases, drug therapy, in particular treatment with glucocorticoids, lead to a decrease in the level of sex hormones. Thus, the use of high doses of glucocorticoids in young men for various diseases causes a decrease in testosterone levels by 47%. In patients with chronic lung diseases, among whom the main group consisted of patients with COPD with low BMD, a decrease in the serum level of 17p-estradiol was revealed, which gave the authors the basis to identify patients with COPD with a low content of 17p-estradiol in special group risk of developing osteoporosis.
Hypo-mobility and decreased muscle strength. It is known that physical activity is necessary to preserve bone mass, the reduction of which (neurological, osteoarticular and other pathologies) contributes to a decrease in BMD. Many patients with COPD with severe respiratory failure, often in hospitals, lead an inactive lifestyle. They have a reduced tolerance to physical activity mainly due to respiratory failure. Shortness of breath in patients with COPD is the main factor that disrupts the quality of life and limits the activity of patients.
NAUMOVANTON VYACHESLAVOVICH
Prevalence and course of osteoporosis in patients with somatic diseases
Moscow - 2010
The work was carried out at the State Educational Institution of Higher Professional Education "Moscow State University of Medicine and Dentistry"
Scientific consultant:
Honored Scientist of the Russian Federation,
Doctor of Medical Sciences, Professor Arkady Lvovich Vertkin;
Official opponents:
Academician of RAMS, professor Martynov Anatoly Ivanovich
Doctor of Medical Sciences, Professor Stryuk Raisa Ivanovna
Doctor of Medical Sciences, Professor Alekseeva Lyudmila Ivanovna
Lead organization:Russian State Medical University. N.I. Pirogov
The defense will take place "___" ______________ 2010 at ___ hours at a meeting of the Dissertation Council D.208.041.01. at the State Educational Institution of Higher Professional Education "Moscow State University of Medicine and Dentistry of Roszdrav" (127473, Moscow, Delegatskaya st., 20/1)
The thesis can be found in the library of the State Educational Institution of Higher Professional Education MGMSU of the Federal Health Service (127206, Moscow, Vuchetich St., 10a)
The abstract was sent "____" ______________ 2010
Scientific Secretary of the Dissertation Council
Doctor of Medical Sciences, Professor Yushchuk E.N.
RELEVANCE OF THE PROBLEM.
According to official statistics, an average of 105.9 cases of fractures of the proximal femur per 100,000 population are diagnosed annually in the Russian Federation in people over 50 years of age (78.8 and 122.5 in men and women, respectively). The leading cause of such fractures is osteoporosis, a progressive systemic skeletal disease characterized by a decrease in bone mass and a violation of the microarchitectonics of bone tissue, leading to an increase in bone fragility and the risk of fractures (WHO, 1999).
According to the report of the International Osteoporosis Foundation (IOF, 2006), after 50 years of complications of this disease, every third woman and every fifth man are diagnosed with this disease, and a third of them die within the first year after an osteoporetic hip fracture. It is for this reason that osteoporosis takes the 4th place in the structure of mortality among the world's population after cardiovascular pathology, diabetes mellitus (DM) and oncological diseases, which indicates the high medical and social significance of the problem (Johnell O. et all, 2004).
At the same time, in the modern literature, when discussing osteoporosis issues, more attention is paid to postmenopausal women, during which excessive activation of bone resorption, induced by estrogen deficiency, leads to a significant loss of bone mineral density (BMD). However, according to E.L. (2005) in 20% of cases the disease occurs in men. Moreover, one third of all cases of osteoporetic hip fractures in the world occur in males, and their immediate and long-term consequences are more severe than in women. Thus, inpatient and outpatient (within a year) mortality after hip fractures in men is 2 times higher than in women (Terrence H. et al., 1997), averaging 40% and 20%, respectively. In addition, about half of men with osteoporosis who have had hip fractures are more disabled and require daily help from medical and social workers. This position is of paramount importance for Russia, where the incidence and premature mortality of men is much higher than in other countries.
According to the official data of the Ministry of Health and Social Development of the Russian Federation, published in 2009, the highest mortality rate in the country is mainly determined by cardiovascular diseases (CVD), which account for 56.6%. At the same time, according to autopsy data, stationary mortality from heart and vascular diseases in Moscow is 48.8%, including more than half of acute vascular accidents (Vertkin A.L., 2009). The situation is further complicated by the fact that patients over 50 years of age who have died from cardiovascular pathology have more than three background or concomitant diseases. Interesting in this regard are the data of Dashdamirov A.Kh., (2005) and Goruleva E.I. (2008) showed that more than 60% of patients with CVD have risk factors for osteoporosis, which is consistent with the results of the study by Farhat G. N., et al. (2007), demonstrating lower BMD values in the vertebral bodies, femoral neck and distal forearm in this category of patients. Moreover, according to U. Sennerby et al. (2007) with cardiovascular pathology there is a manifold increase in the risk of fracture of the proximal femur, and according to Vasan R.S., et al. (2003) among similar patients, the majority have a high level of proinflammatory cytokines in combination with osteoporosis. These data allowed Marcovitz P.A. et all (2005) believe that loss of BMD is one of the predictors of CVD development.
It is well known that one of the main underlying diseases in cardiovascular pathology is type 2 diabetes. According to A.L. Vertkin. (2009) among 3239 autopsies of patients who died in a multidisciplinary hospital, 19% had diabetes, including 97, 1% had type 2. About 50 years ago, Albrigt and Reifehstein hypothesized that diabetes may cause a decrease in bone mass. Today this condition is called diabetic osteopenia. It is especially pronounced in men with cardiovascular pathology (Ermachek E.A., 2006). Diabetes mellitus of the second type develops, as a rule, after 30 years, when the age-related decrease in the secretion of total testosterone begins in men, which leads to the onset of androgen deficiency, which, according to Amin S. et all, (2000) and Khaibulina E.T. (2007) is the main cause of osteoporosis. In the study of Dedov I.I. (2005) and Khalvashi R.Z., (2008) it is shown that approximately 2/3 of men with hypogonadism are diagnosed with reduced bone density, including one third - osteoporosis.
The second place in the country in terms of mortality is occupied by oncological diseases (Ministry of Health and Social Development, 2009). At the same time, according to the autopsy data of deceased patients in general somatic departments, malignant neoplasms are diagnosed in 6 - 8% of cases (Vertkin A.L., 2009). Cancer patients (including those already conditionally cured) are also at risk of developing osteoporosis and its complications. There are a number of explanations for this, including the forced intake of cytostatics, hormonal levels changed after surgery, etc. (NP Makarenko, 2000). It is important to emphasize that the earlier the influence of unfavorable factors on the bone is observed, the higher the risk of developing osteoporosis and fractures already at a young age (Mahon S., 1998).
Another reason contributing to the high incidence of osteoporosis and associated fractures is chronic obstructive pulmonary disease (COPD). This pathology is in 13% of cases the cause of death in patients in a general hospital (Vertkin A.L., 2009).
According to epidemiological studies by Van Staa T.P. et al. (2001) conducted for 5 years in patients with COPD, in about half of the cases, either osteopenia or osteoporosis is diagnosed. The authors explain the obtained results primarily by common risk factors for COPD and osteoporosis (smoking, vitamin D and body weight deficiency), long-term intake of glucocorticosteroids, activation of bone resorption under the influence of mediators of systemic inflammation: TNF-α and interleukin-6 (Eid AA, et al. 2005).
Thus, the data presented provide convincing evidence of the role of somatic pathology in patients with osteoporosis. This is of particular relevance in connection with the increase in the number of people over the age of 65 with a high comorbid background. According to experts' forecasts, the costs of these individuals for the treatment of osteoporotic fractures and, above all, of the femoral neck will increase progressively, and by 2025 they will amount to 31.8 billion euros (IOF, 2006).
To prevent such an unfavorable situation for any society, a global strategy is the timely diagnosis and prevention of the disease among the general population (IOF, 2001-2007), as well as identifying patients who are at high risk of developing fractures (Michigan Quality Improvement Consortium; 2008).
In this regard, it is of interest to identify early markers of osteoporosis using simple clinical manipulations (IOF, 2005). Among them are the studies by Mohammad A.R. et al., (2003) demonstrated that patients with missing teeth have low BMD values. This led the authors to assume that tooth loss due to periodontal disease can be considered a marker of systemic loss of BMD. This can be confirmed by the still few clinical studies showing that women with chronic generalized periodontitis have more than 3 times higher risk of osteoporosis than patients without significant lesions of the oral mucosa (Gomes-Filho S. et al. , 2007). Similar data were obtained in the studies of Wactawski-Wende J. et al., (2005), according to which menopausal women had a significantly higher risk of chronic generalized periodontitis with a reduced BMD.
Traditionally, the diagnosis, prevention and treatment of osteoporosis are a priority, first of all, for rheumatologists, less often for endocrinologists and gynecologists. This is due to the fact that most studies on the effectiveness of treatment of osteoporosis with antiresorptive drugs were carried out mainly in the population of postmenopausal women, and the criteria for exclusion were severe somatic diseases (Povoroznyuk V.V., 2003).
At the same time, the Russian health care system provides the primary health care sector with ample opportunities to implement a set of measures for primary and secondary prevention of diseases in most patients (L.I. Benevolenskaya, 2007; I.V. Galkin et al., 2009). Therefore, the transfer of the center of gravity for the early detection of osteoporosis to local polyclinics will significantly improve the provision of medical care for this and highly common pathology. This study is devoted to the development of effective screening programs, clinical features, prevention and treatment of osteoporosis in somatic patients.
PURPOSE OF THE STUDY
Determination of the prevalence, clinical and prognostic value of osteoporosis and methods of its optimal drug correction in patients with somatic pathology.
RESEARCH OBJECTIVES
Develop a program for the detection, prevention and treatment of osteoporosis based on multidisciplinary medical institutions
To conduct a retrospective analysis of the features of the comorbid background in patients who have undergone atraumatic fracture of the proximal femur.
To carry out a comparative histomorphological analysis of the state of bone tissue in patients with somatic pathology.
To assess the prevalence of osteopenia and osteoporosis in patients with comorbid conditions
Clarify the gender characteristics of bone mineral density loss in patients with somatic diseases.
To study the role of osteoporosis screening in patients with periodontal disease as an early marker of BMD loss
To determine the effectiveness of programs for the prevention and treatment of osteoporosis in patients with somatic diseases.
For the first time, osteoporosis was screened on a large sample of patients with somatic pathology. It has been shown that out of 8600 patients with various diseases of internal organs, osteoporosis is diagnosed in 34.3% of cases, while out of 1200 patients without chronic somatic diseases, it was detected only in 18.6% of cases. At the same time, the loss of BMD is observed in 77.5% of patients with somatic pathology.
It was revealed that OP is more often detected in patients with cardiovascular pathology, COPD, and oncological diseases. Osteopenia is more commonly diagnosed in patients with type 2 diabetes. The severity of BMD loss in any somatic disease significantly exceeds that in the control group.
It was stated that the most significant risk factors for osteoporosis, both in men and women, are hypogonadism in combination with somatic pathology (reliability of the factor p = 0.013 and p = 0.014, respectively).
It has been shown that almost all patients with atraumatic fracture of the proximal femur have chronic somatic diseases, at different times before the fracture, all of them have repeatedly consulted a therapist. Atraumatic fracture of the proximal femur occurs more often in women (the ratio of men to women is 1: 3), mainly in old age (77.3 ± 7.5), but in men, almost 7 years earlier. These patients, in the overwhelming majority of cases, undergo surgical procedures depending on the type of traumatic injury.
A histomorphometric study in the bone tissue of patients who died not from somatic diseases revealed a predominance of the matrix over the number of resorption cavities, while in patients who died from somatic diseases, an inverse relationship was observed, and a significant decrease in newly formed bone units was also noted (Haversseye systems). These ratios remain valid even when adjusted for age. This is evidence of a significant loss of bone mass and density in patients with somatic pathology, in contrast to patients whose death did not occur from somatic diseases.
For the first time, as an early clinical marker of OP, it was proposed to consider the pathology of the periodontal complex. It was determined that in the presence of osteoporosis, periodontal damage is practically independent of the degree of BMD loss, while in patients with osteopenia, and to a greater extent in patients without BMD loss, the severity of periodontal damage is proportional to the BMD level.
The study revealed that the prevention of osteoporosis in patients with somatic pathology (education of patients, lifestyle changes, prescription of combined calcium and vitamin D3 preparations) leads to an increase in BMD by more than 7% in the first two years. While only education and lifestyle changes are accompanied by additional loss of BMD and the development of OP in almost 15% of patients in the next two years.
The most effective antiresorptive drugs for the treatment of AP in patients with somatic pathology are ibandronic acid, semi-synthetic salmon calcitonin, and alendronic acid. Patients with somatic pathology and OP who do not receive antiresorptive drugs will additionally lose 5.6% of BMD in the next two years (р
PRACTICAL SIGNIFICANCE.
For the first time, on the basis of a multidisciplinary hospital, a city office of osteoporosis was created for screening, diagnostics and treatment of osteoporosis in patients with somatic pathology, equipped with a bone densitometer, which allows performing X-ray, two-photon absorptiometry of the distal forearm.
For the first time, “additional” risk factors for AP in patients with somatic diseases have been identified. Thus, inadequate blood pressure control, hypercholesterolemia and organ lesions in CVD (LVH, impaired myocardial contractility) are prognostically less favorable for BMD loss. In patients with COPD, the presence of chronic obstructive bronchitis and the use of systemic steroids are also unfavorable for the course of AP, however, the use of corticosteroids contributes to some preservation of BMD. In patients with type 2 diabetes, age, as well as inadequate control of carbohydrate metabolism, contribute to an additional loss of BMD. In case of oncological pathology, patients who have undergone radical operations on the thyroid gland, mastectomy, as well as with the localization of a malignant formation in the kidney or prostate gland, require special attention of doctors in terms of identifying and correcting osteoporotic changes in bone tissue.
In the structure of somatic pathology of patients who have undergone an atraumatic fracture of the proximal femur, cardiovascular pathology, type 2 diabetes and COPD prevail, their combination is more often (86.3%). This is reflected in the prognosis of the disease, both in the early inpatient and in the long-term periods. Thus, hospital mortality is 6.2%, and every fourth dies within the first year after a fracture as a result of the development of acute coronary events, pulmonary embolism and erosive and ulcerative bleeding from the upper digestive tract.
The study revealed that, despite the slightly higher prevalence of osteoporosis and osteopenia in menopausal women, in the presence of androgen deficiency in men, BMD losses are more significant than in women with hypogonadism.
It was revealed that in patients with osteoporosis, the state of the periodontal complex is characterized by a significantly greater lesion than in patients with osteopenia and without loss of BMD. Computed radiovisiography can serve as a screening tool for detecting low BMD. A moderate, significant correlation was found between the optical density of the alveolar bone and the BMD of the peripheral skeleton, measured by bone densitometry (r = 0.4, p = 0.002).
Read also ...