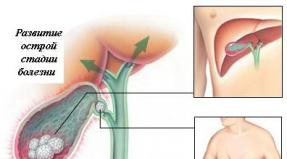
Keloid scar Consequences of thermal and chemical burns, frostbite, wounds. What it is
A keloid scar (ICD 10) is a scar formation that forms on an area of \u200b\u200bthe affected skin. The damage must be treated, otherwise traces may remain for life. A keloid scar also indicates the rapid healing of destroyed skin tissues.
Keloid scar according to the microbial code 10 is classified as a physiological phenomenon. This is the result of the restoration of artificially deformed tissues. Often scars heal and become invisible, but keloid scars are distinguished by a pronounced character and appearance.
A keloid is a dense growth that may outwardly resemble a tumor, it has the following features:
- The scar is located outside the boundaries of the damaged area. Expands horizontally.
- A keloid is a cicatricial scar that is characterized by acute pain, itching. A striking example is the feeling of skin tightening.
- If over time it becomes almost invisible, then the colloidal does not change color or size. This is due to the fact that blood vessels grow inward.
Causes and symptoms of education
Even minor skin defects lead to the formation of painful scars. Among the main reasons are:
- Self-healing wound. If the edges of the incision are not connected correctly, the skin is deformed and the disease cannot be avoided. The doctor can also make this mistake.
- Keloid appears as a consequence of infection. Disinfection and the use of appropriate products is a prerequisite for safe wound management.
- As confirmed by the microbial code 10, it is formed after too much tension on the skin during suturing. This spoils the appearance initially and later becomes a factor of destructive influence.
- Medical examinations identify keloids as a result of hormonal imbalances. Including among the reasons, immunodeficiency stands out.

International classification disease takes into account hereditary predisposition. The abundance of scars in relatives may indicate a high probability of the formation of a keloid scar.
Possible complications
The international classifier does not record keloids as dangerous diseasesthat constitute a threat and lead to serious complications. This will not cause a future tumor, malignant formation, which is a risk to life.

Scar removal and alteration is initiated for two reasons:
- Aesthetic. It looks ugly on an open area of \u200b\u200bthe skin. The scar does not disguise itself as a tan and when germinating blood vessels stands out on the body.
- Practical. Scars located at the bend of the joints hinder movement. Wearing tight-fitting clothing causes discomfort and itching from rubbing.
Prevention of the appearance
You can prevent the appearance of a keloid in the following ways:
- Bandages. Special dressings that create strong pressure localize the spread. However, not every wound allows for such solutions.
- Balanced treatment. A timely visit to a doctor will help disinfect the wound and develop individual program recovery. The use of vinegar and other harsh agents leads to side effects.
- Caution. It is impossible to squeeze out the abscess or massage the scar due to itching. This speaks of an inflammatory process, so it is worth contacting a specialist.
- Cold rest. Baths, saunas and high temperatures are contraindicated in patients with keloids.
Most of the deformation of the scars is a consequence of wound infection. When you receive an abrasion or mechanical damage to the skin, the main thing is to consult a doctor in time, do not load deformed tissues and do not self-medicate.
Rough scars and scars on the face or body today no longer serve as an adornment for real men and, even more so, women. Unfortunately, the possibilities of modern medical cosmetology do not allow to completely get rid of cicatricial defects, suggesting only to make them less noticeable. The scar correction process takes persistence and patience.
"Scar" and "scar" are synonymous words. A scar is a household name for a scar. Scars on the body are formed as a result of the healing of various skin lesions. Exposure to mechanical (trauma), thermal (burns) agents, skin diseases (post-acne) lead to disruption of the physiological structure of the skin and its replacement by connective tissue.
Scars can sometimes be very insidious. With normal physiological scarring, the skin defect shrinks and turns pale over time. But in some cases, scarring is pathological character: The scar becomes bright purple in color and increases in size. In this case, immediate specialist assistance is needed. The problem of scar correction is dealt with in the community of dermatocosmetologists and plastic surgeons.
Scar formation.
In its formation, the scar goes through 4 stages successively replacing each other: I - the stage of inflammation and epithelialization.It lasts from 7 to 10 days from the moment the injury occurs. It is characterized by a gradual decrease in swelling and inflammation of the skin. Granulation tissue is formed, bringing the edges of the wound closer together, the scar is still absent. If there is no infection or dehiscence of the wound surface, then the wound heals by primary intention with the formation of a barely noticeable thin scar. In order to prevent complications at this stage, atraumatic sutures are applied, sparing tissues, daily dressings are performed with local antiseptics. Physical activity is limited to avoid dehiscence of the wound edges. II - stage of formation of a "young" scar.
Covers the period from the 10th to the 30th day from the moment of injury. It is characterized by the formation of collagen-elastin fibers in the granulation tissue. The scar is immature, loose, easily stretchable, bright pink in color (due to increased blood supply to the wound). At this stage, secondary wound trauma and increased physical exertion should be avoided. III - stage of "mature" scar formation.
Lasts from the 30th to the 90th day from the day of the injury. Elastin and collagen fibers grow into bundles and line up in a specific direction. The blood supply to the scar decreases, which causes it to thicken and turn pale. At this stage, there are no restrictions on physical activity, but repeated injury to the wound can cause the formation of a hypertrophic or keloid scar. IV - stage of the final transformation of the scar.
Starting from 4 months after injury and up to a year, the final maturation of the scar occurs: the death of blood vessels, tension of collagen fibers. The scar thickens and turns pale. It is during this period that the doctor understands the condition of the scar and the further tactics of its correction.
It is not possible to get rid of scars once and for all. With the help of modern techniques, you can only make a rough, wide scar more cosmetically acceptable. The choice of method and the effectiveness of treatment will depend on the stage of scar defect formation and on the type of scar. In this case, the rule applies: the earlier you seek medical help, the better the result will be.
A scar is formed as a result of a violation of the integrity of the skin (surgery, trauma, burns, piercing) as a result of the processes of closing the defect with new connective tissue. Superficial damage to the epidermis heals without scarring, that is, the cells of the basal layer have good regenerative capacity. The deeper the damage to the layers of the skin, the longer the healing process and the more pronounced the scar. Normal, uncomplicated scarring results in a normotrophic scar that is flat and the color of the surrounding skin. Violation of the course of scarring at any stage can lead to the formation of a rough pathological scar.
Types of scars.
Before choosing a method of treatment and the optimal timing of a particular procedure, you should determine the type of scars.Normotrophic scars usually do not cause great distress to patients.They are not so noticeable, so their elasticity is close to normal, they are pale or flesh-colored and are at the level of the surrounding skin. Without resorting to radical methods of treatment, such scars can be safely removed using microdermabrasion or chemical surface peeling.
Atrophic scars can occur as a result of acne or poor-quality removal of moles or papillomas. Stretch marks (striae) are also this type of scar. Atrophic scars are located below the level of the surrounding skin, characterized by tissue laxity resulting from a decrease in collagen production. Lack of skin growth leads to the formation of pits and scars, creating a visible cosmetic defect. Modern medicine has a lot in its arsenal effective ways elimination of even sufficiently extensive and deep atrophic scars.
Hypertrophic scars are pink in color, limited to the damaged area and protrude above the surrounding skin. Hypertrophic scars can partially disappear from the surface of the skin within two years. They respond well to treatment, so you shouldn't wait for them to disappear spontaneously. Small scars can be treated with laser resurfacing, dermabrasion, chemical peeling. The introduction into the scar area leads to positive results hormonal drugs, diprospan and kenalog injections. Electro- and phonophoresis with kontubex, lidase, hydrocortisone give a stable positive effect in the treatment of hypertrophic scars. maybe surgery, in which scar tissue is excised. This method gives the best cosmetic effect.
Keloid scars have a sharp border, protrude over the surrounding skin.Keloid scars are often painful, itching and burning are felt in the places of their formation. This type of scars is difficult to treat, and recurrence of even larger keloid scars is possible. For all the complexity of the task, aesthetic cosmetology has many examples of a successful solution to the problem of keloid scars.
Features of keloid scars.
The success of the treatment of any disease largely depends on the correct diagnosis. This rule is no exception in the case of elimination of keloid scars. To avoid mistakes in treatment tactics, it is possible only by clearly defining the type of scar, etc., in terms of external manifestations, keloid scars often resemble hypertrophic scars. A significant difference is that the size of hypertrophic scars coincides with the size of the damaged surface, while keloid scars extend beyond the boundaries of the injury and in area may exceed the size of the traumatic skin injury. The usual places of occurrence of keloid scars are the chest area, auricles, less often the joints and the face area. Keloid scars go through four stages in their development.Epithelialization stage. After injury, the damaged area is covered with a thin epithelial film, which thickens, coarsens, becomes pale in color within 7-10 days and remains in this form for 2-2.5 weeks.
Swelling stage. At this stage, the scar enlarges, rises above the adjacent skin, and becomes painful. In the course of 3-4 weeks, the painful sensations weaken, and the scar acquires a more intense reddish color with a cyanotic shade.
Compaction stage. There is a compaction of the scar, in some places there are dense plaques, the surface becomes bumpy. The external picture of the scar is a keloid.
Softening stage. At this stage, the scar finally acquires a keloid character. It is characterized by pale color, softness, mobility and painlessness.
When choosing treatment tactics, one proceeds from the age of the scars. Keloid scars from 3 months to 5 years of existence (young keloids) are actively growing, they are distinguished by a smooth shiny surface, red in color with a cyanotic shade. Scars older than 5 years (old keloids) turn pale, acquire a wrinkled uneven surface (sometimes the central part of the scar sinks).
Keloid scars can be caused by surgery, vaccinations, burns, insect or animal bites, and tattoos. Such scars can occur even without traumatic injury. In addition to significant aesthetic discomfort, keloid scars give patients unpleasant sensations of itching and soreness. The reason for the development of this particular type of scars, and not hypertrophic ones, has not been established by doctors at the moment.
A little about scarring.
Information about scars will be incomplete if you pass over in silence such a procedure as scarification or scarification - the artificial application of decorative scars to the skin. For some, this newfangled direction of body art is a way to disguise existing scars, for others it is an attempt to give their appearance masculinity and brutality. Unfortunately, the thoughtless fascination of young people with such procedures, as well as other artificial skin lesions (tattoos, piercings), leads to irreversible consequences. Fashion passes, but scars remain forever.Severe skin pigmentation Definite localization of initial lesions (deltoid muscle region, chest, earlobe) Pregnancy Puberty.
Pathomorphology
Histological examination reveals elongated convoluted bundles of eosinophilically colored hyalinized collagen, thinning of the papillae of the dermis and a decrease in the elasticity of the fibers. Morphological basis
is overgrowing immature connective tissue with a large number of atypical giant fibroblasts that are in a functionally active state for a long time. IN
keloids
few capillaries, mast and plasma cells.
Keloid: Signs, Symptoms
Clinical picture

Pain Soreness Hyperesthesia Itching Hard, smooth, well-defined scars rising above the skin surface At the onset of the disease, there may be pallor or slight erythema of the skin The scar covers a larger area than the initial damage Even after years
continue to grow and can form claw-like outgrowths.
Keloid scar symptoms
Keloid and hypertrophic scars are accompanied by redness (hyperemia), painful sensations after pressing on the scar. In this place, the tissues are highly sensitive. The scars begin to itch. Keloids develop in two stages:
- Active is characterized by the dynamic growth of keloid tissues. This is accompanied by itching, numbness of the affected areas, and tissue soreness. This stage begins with the epithelialization of the wound and lasts up to a year.
- In the inactive period, the final scar formation occurs. It is called stabilized, acquiring normal skin color. The resulting scar does not bother the owner, but it looks unaesthetic in open areas of the body.
There are two types of keloids. True ones rise above the skin and are whitish or pink in color. Scars are dense, with a smooth, shiny surface with a minimum content of capillaries.
The formation of keloids is accompanied by the following symptoms:
- hyperemia (redness) in the area of \u200b\u200bthe scar;
- painful sensations when pressed;
- hypersensitivity in the area of \u200b\u200baffected tissues;
- itching when scratching.
The development of keloids goes through two stages - active and inactive.
During the active stage, a dynamic growth of keloid tissue occurs, which causes physical discomfort for the patient: itching, soreness and / or numbness of the affected tissues. This stage begins from the moment of epithelialization of the wound and can last up to 12 months.
The inactive stage ends with the final formation of the scar. Such a keloid is called otherwise stabilized, since its color resembles the natural color of the skin, and the scar itself does not cause much concern, except for an unaesthetic appearance, especially in open areas of the body.
Keloid: Diagnosis
Distinguish between true (spontaneous) and false keloid.

Differential diagnosis
Hypertrophic scars Dermatofibroma Infiltrating basal cell carcinoma (confirmed by biopsy).
Conservative treatment
Keloid scar - how to get rid of it with conservative treatment? First, a diagnosis is carried out, a biopsy is prescribed to exclude a malignant neoplasm.
Treatment begins with conservative techniques. They help well if the scars are not yet old, formed no more than a year ago.

During compression, pressure is applied to the affected area. The growth of the keloid is stopped by squeezing. The nutrition of the scar tissue is blocked, its vessels are compressed. All this contributes to stopping the proliferation.
Ointment for keloid scars is only an auxiliary method. As an independent direction of funds is rarely used. Ointments are usually prescribed as additional drugs with antibacterial, anti-inflammatory and circulation-restoring effects.
As a cosmetic correction of acne-keloid, different methods are used: dermabrasion, peels. They are all aimed at change appearance scars.
Mesotherapy and other cosmetic methods are carried out only for the upper skin layer, in order to avoid the proliferation of connective tissue. Correction is indicated only for old scars.
In other cases, three main conservative methods are most commonly used to remove them. The first way how a keloid scar is removed: treatment with silicone plates.
They are used immediately after the first wound healing. Silicone plates are mainly indicated for people with a tendency to form keloids.
The essence of the technique is based on squeezing the capillaries. As a result, collagen synthesis decreases and tissue hydration stops. A special patch with plates is used daily from 12-24 hours. The course of therapy is from 3 to 18 months. Compression is a variety this method.
Method two: Treatment of keloid scars with corticosteroids is indicated for local use. An injection is made into the bulge, which includes a suspension of triamcinolone acetonide. It is allowed to inject from 20 to 20 milligrams of the drug per day, 10 mg is consumed for each scar.
The purpose of the injections is to reduce collagen production. At the same time, the division of fibroblasts that produce it decreases, and the amount of collagenase increases.
Treatment is most effective for non-persistent scars. In this case, small doses are sufficient for therapy.
After a month, the course of treatment is repeated until the scars are even with the skin surface.
The third main method of how to get rid of keloid scars is called cryodestruction. This is a destructive effect on scar tissue with liquid nitrogen. As a result, a crust appears on the treated area.
Healthy tissues are formed under it. After the end of the process, the crust falls off on its own, leaving an almost imperceptible mark. Cryodestruction is effective only for new keloid and hypertrophic scars.
Aggressive removal of keloid scars is performed in two ways - surgically or using a laser. In the first case, during the operation, not only the overgrown tissues are excised, but also the affected area of \u200b\u200bthe skin.
The surgical method has its drawbacks - there is a high probability of the formation of new keloid scars.
This risk is somewhat reduced by removing the affected skin area. Nevertheless, relapses are observed in 74-90 percent of cases. Surgery is indicated only when conservative treatment turned out to be ineffective.
With the help of laser therapy, keloid scars that have minimally touched the surrounding tissues are removed or cauterized. Correction is applied in complex treatment and is combined with corticosteroid and topical methods. In laser therapy, relapses are much less common - in 35-43 percent.

Treatment of a keloid in the ear occurs according to a certain scheme. First, diprospan or kenolog-40 is appointed.
Injections are given into the scar tissue. A month after the start of treatment, laser therapy is performed using Bucca rays.
The patient wears a special squeezing clip on the ear (at least 12 hours daily).
At the end of therapy, phono- and electrophoresis with collagenase or lidase is prescribed to consolidate the effect. At the same time, ointments and gels are prescribed (Lyoton, Hydrocotisone, etc.).
If after this the growth of scar tissue does not stop, then close-focus X-ray therapy is added to the treatment. In severe and difficult cases, methotrexate is given.
A keloid scar after a cesarean can be treated in many ways. In some cases, deep chemical peeling helps to get rid of keloid scars.
First, the scar is treated with fruit acids. After that, chemicals are applied.
This method is ineffective, but also the most budgetary.
For the treatment of a keloid scar after removal of a mole or caesarean section plates and gels containing silicone are prescribed. There are many collagenase-based anti-scar products.
Hyaluronidase preparations are used. Hormone-based products with vitamins and oils help to eliminate keloid scars.
To remove mature scars, physiotherapy is prescribed: phono-electrophoresis. These are effective and painless procedures. In extreme cases, plastic surgery or laser resurfacing is done. A more gentle method is microdermabrasion. During the procedure, microparticles of aluminum oxide are used.

There are many ways to treat keloid scars using traditional methods. The scars are not completely removed, but they become less visible.
Plant-based products are used. For example, 400 g is taken sea \u200b\u200bbuckthorn oil and mixed with 100 g of beeswax.
The solution is heated in a water bath for 10 minutes. Then a gauze napkin is dipped into the mixture and applied to the scar.
The procedure is performed twice a day. The course of treatment is three weeks.
To remove scars, compresses are made with camphor, in which the bandage is moistened. Then he applies to the scar. The compress is done daily for a month. Only then will the result be seen.
You can make a tincture of delphinium. The roots of the plant are highly crushed. Alcohol and water are added to them, mixed in equal proportions. The container is removed for two days in a dark place. Then a gauze cloth is soaked in the liquid and applied to the keloid scar.
An ointment based on the Japanese Styphnolobia is made independently. A couple of glasses of the plant's beans are crushed and mixed with badger or goose fat in equal proportions.
The mixture is infused for 2 hours in a water bath. Then, with an interval of a day, it is heated twice more.
After that, the mixture is boiled, mixed and transferred to a ceramic or glass jar.
Keloid scars do not pose a threat to health or life, but they can cause nervous disorders due to the unaesthetic appearance of the body. In the early stage, neoplasms are treated much easier than in the neglected version.
According to statistics, keloid scars are not very common - only 10 percent of cases. This disease is most susceptible to women. To prevent scarring, you must follow all the prescriptions of doctors and not self-medicate.
The nature of the keloid is not fully understood, therefore, to date, a universal treatment method has not been developed. The methods are chosen by the doctor individually for each patient, depending on clinical picture diseases.
Treatment methods can be divided into conservative and aggressive (radical).
It is preferable to start with conservative ones, especially if the scars are young - no more than one year old. Three methods are recognized as the most effective:
- using a silicone coating / gel;
- corticosteroid injection therapy;
- cryotherapy.
Application of silicone plates
It is necessary to start using silicone plates in the form of a patch immediately after the initial wound healing in people with a predisposition to the development of keloids.
The mechanism of this technique is based on squeezing the capillaries, reducing collagen synthesis and hydration (hydration) of the rumen. The patch must be used 12 to 24 hours a day.
The period of treatment is from 3 months to 1.5 years.
A variation of this method of treatment can be considered compression (squeezing), as a result of which the growth of the keloid stops, nutrition is blocked and the vessels of the scar are compressed, which leads to a cessation of its growth.
Corticosteroid injections
This technique is used locally. With the help of an injection, a suspension of triamcinolone acetonide is injected into the rumen.
You can enter 20-30 mg of the drug per day - 10 mg for each scar. Treatment is based on reducing collagen synthesis.
At the same time, the division of fibroblasts that produce collagen is inhibited, and the concentration of collagenase, an enzyme that breaks down collagen, increases.
Low-dose treatment is effective for fresh keloid scars. After 4 weeks, the treatment is repeated until the scars are compared to the skin surface. If there is no therapeutic effect, a triamcinolone suspension containing 40 mg / ml is used.
Steroid treatment can cause complications:
Treatment
Management tactics
Local injections of HA are most effective.Pressure on the damaged area prevents the development of
Bandages are used that create a pressure of up to 24 mm Hg above the injury site. Art. , within 6-12 months. The bandage can be removed for no more than 30 min / day. Radiation therapy in combination with GC - if other methods of treatment are ineffective.
Surgery
indicated only in case of extensive lesion and ineffectiveness of local treatment of HA. There is a high frequency of relapses, therefore, surgical treatment is recommended to be carried out no earlier than 2 years after education.
immediately preventive treatment (as in the emerging
Drug therapy
In one day, the drug can be injected into 3 scars (10 mg for each scar) The needle should be injected in different directions for better distribution of the drug The effectiveness of the method is higher with fresh keloid scars The treatment is repeated every 4 weeks until the scars are compared with the skin surface.If there is no effect, you can apply a suspension of triamcinolone containing 40 mg / ml with surgical excision.
keloids
you can apply a mixture of p - ra triamcinolone (5-10 mg / ml) with local anesthetics. For the prevention of relapses after surgery - HA injections into the area of \u200b\u200bscar excision after 2–4 weeks and then 1 r / month for 6 months.
Course and prognosis
Under the influence of triamcinolone
decrease in 6–12 months, leaving flat, light scars.
ICD-10 L73. 0 Acne keloid L91. 0 Keloid scar.
Tags:
Did this article help you? Yes -0 No -0 If the article contains an error Click here 47 Rating:
Prevention
To reduce the risk of recurrence after surgery to remove the keloid, it is customary to take preventive measures already in the process of forming a new scar (for 10-25 days).
All therapeutic (conservative) methods are used as preventive measures. After the operation, you must constantly use sunscreen with high level protection.
Includes: conditions that warrant observation, hospitalization or other obstetric care for the mother, as well as for a caesarean section before labor begins
Excludes: listed conditions with obstructed labor (O65.5)
- double uterus
- bicornuate uterus
Medical care for the mother with:
- polyp of the body of the uterus
- uterine fibroid
Excludes: maternal care for cervical tumor (O34.4)
Medical care for the mother with a scar from a previous cesarean section
Excludes: vaginal delivery after previous caesarean section NOS (O75.7)
Suturing the neck with a circular suture with or without mention of cervical insufficiency
Shirodkar suture with or without mention of cervical insufficiency
Medical care for the mother with:
- polyp of the cervix
- previous surgery on the cervix
- stricture and stenosis of the cervix
- tumors of the cervix
Providing medical care mothers with:
- infringement of the pregnant uterus
- prolapse of a pregnant uterus
- retroversion of the pregnant uterus
Medical care for the mother with:
- previous vaginal surgery
- dense hymen
- vaginal septum
- vaginal stenosis (acquired) (congenital)
- vaginal stricture
- vaginal tumors
Excludes: medical care for the mother with varicose vaginal veins during pregnancy (O22.1)
Medical care for the mother with:
- fibrosis of the perineum
- previous surgery on the perineum and vulva
- rigid perineum
- vulvar tumors
Excludes: maternal care for varicose veins of the perineum and vulva during pregnancy (O22.1)
Medical care for the mother with:
- cystocele
- plastic surgery of the pelvic floor (with a history)
- saggy belly
- rectocele
- rigid pelvic floor
In Russia International classification of diseases 10th revision ( ICD-10) adopted as a single normative document to take into account the incidence, the reasons for the population's appeals to medical institutions all departments, causes of death.
ICD-10 introduced into healthcare practice throughout the Russian Federation in 1999 by order of the Ministry of Health of Russia dated 05/27/97. No. 170
The publication of a new revision (ICD-11) is planned by WHO in 2022.
Source: mkb-10.com
Postoperative uterine scar requiring maternal medical attention
Definition and background [edit]
A scar (scars) is a dense formation consisting of hyalinized connective tissue rich in collagen fibers, resulting from reparative tissue regeneration in violation of its integrity.
A scar on the uterus is the area of \u200b\u200bthe uterus in which previous surgical interventions were performed (cesarean section, myomectomy, reconstructive plastic surgery)
According to various authors, a scar on the uterus after cesarean section is present in 12-16% of pregnant women, and every third abdominal birth is subsequently repeated. The prevalence of cesarean section in the Russian Federation over the past 30 years (since 1980) has increased 3 times and is 22-23%. The number of pregnant women with uterine scar after myomectomy is increasing. If this is done by laparoscopic or laparotomic access in the presence of an interstitial component, a scar will also form. The incidence of inconsistent scars after myomectomy reaches 21.3%.
Wealthy scar on the uterus.
Inconsistent scar on the uterus.
a) Localization of the scar on the uterus after cesarean section:
- in the lower uterine segment;
- partly in the lower segment, partly in the body (after an isthmic-corporal incision in the uterus);
b) Scar on the uterus after myomectomy before and during pregnancy:
- without opening the uterine cavity;
- with the opening of the uterine cavity;
- scar on the uterus after removal of the subserous-interstitial node;
- scar on the uterus after removal of the cervical fibroids.
c) A scar on the uterus after perforation of the uterus [with intrauterine interventions (abortion, hysteroscopy)].
d) A scar on the uterus after an ectopic pregnancy, located in the interstitial section of the fallopian tube, in the cervix after removal of the cervical pregnancy.
e) Scar on the uterus after reconstructive plastic surgery (Strassmann's operation, removal of the rudimentary horn of the uterus, plastic isthmus for an insolvent scar on the uterus after cesarean section).
A scar on the uterus is formed as a result of cesarean section, after myomectomy, perforation of the uterus, tubectomy. Scarring is a biological mechanism for the healing of damaged tissues. Healing of the dissected uterine wall can occur through both restitution (full regeneration) and substitution (defective). With full-fledged regeneration, wound healing occurs due to smooth muscle cells (myocytes), with substitution - due to bundles of coarse fibrous connective, often hyalinized tissue.
Postoperative uterine scar requiring maternal care: Diagnosis [edit]
Informative methods for diagnosing the condition of a scar on the uterus in a non-pregnant woman are hysterography, or better, hysteroscopy, ultrasound examination (ultrasound).
Hysterography produced on the 7-8th day of the menstrual cycle, but not earlier than 6 months after the operation in frontal and lateral projections. The method allows you to study changes in the inner surface of the postoperative scar on the uterus. The inconsistency of the postoperative scar is indicated by: a change in the position of the uterus in the small pelvis (significant anterior displacement of the uterus, jagged and thinned contours of the inner surface of the uterus in the area of \u200b\u200bthe alleged scar, "niches" and defects in its filling).
Hysteroscopy is performed on the 4-5th day of the menstrual cycle, when the functional layer of the endometrium is completely rejected, and the underlying tissue is visible through the thin basal layer. Scar failure is usually indicated by local retraction or thickening in the area of \u200b\u200bthe scar. The whitish color of the scar tissue, the absence of blood vessels indicate a pronounced predominance of the connective tissue component, and retraction - about the thinning of the myometrium as a result of defective regeneration. An unvisualized uterine scar and a scar with a predominance of muscle tissue indicate its anatomical and morphological usefulness.
Ultrasound procedure... Echoscopic signs of uterine scar failure include: uneven outline along the back wall of a filled bladder, thinning of the myometrium, discontinuity of the contours of the scar, a significant number of echo-dense inclusions (connective tissue). With two-dimensional ultrasound, pathological changes in the area of \u200b\u200bthe scar on the uterus are found much less often than with hysteroscopy (56% and 85%, respectively). But with the advent of the Doppler method and 3D reconstruction, the informativeness of ultrasound for assessing the state of the scar on the uterus has significantly increased, since it became possible to assess the hemodynamics of the scar (the development of the vascular network). The results obtained from additional methods for diagnosing the state of a scar on the uterus outside of pregnancy are entered into an outpatient card and taken into account when deciding on the possibility of planning a subsequent pregnancy.
In the presence of an inconsistent scar on the uterus at the stage of pregnancy planning, in order to prevent its rupture during subsequent pregnancy, a reconstructive operation is indicated - plastic isthmus of the uterus, which is performed in a gynecological hospital by a highly qualified gynecological surgeon using laparotomic or laparoscopic access.
Careful selection of pregnant women for spontaneous childbirth.
Thorough cardiotocographic and ultrasound control during spontaneous labor.
Adequate pain relief during spontaneous labor.
Excision of an inconsistent scar on the uterus with a second cesarean section.
Postoperative uterine scar requiring maternal care: Treatment [edit]
Management of pregnant women with a scar on the uterus after cesarean section
Careful collection of anamnesis, including information about a previous caesarean section on the basis of a discharge from an obstetric hospital.
Information about uterine scar studies performed outside and during pregnancy.
Parity: whether there was a spontaneous delivery before surgery; the number of pregnancies between the operation and the actual pregnancy, how they ended (abortion, miscarriage, missed pregnancy).
The presence of living children, whether there have been stillbirths and deaths of children after a previous birth.
b) Physical examination
Palpation examination of the scar on the anterior abdominal wall and on the uterus; measuring the size of the pelvis and the estimated weight of the fetus; assessment of the state of the birth canal and readiness of the body for childbirth at 38-39 weeks of gestation.
c) Instrumental research methods
Ultrasound of the fetus using Dopplerometry of the vessels of the umbilical cord, aorta, middle cerebral artery of the fetus and placenta, starting from the end of the second trimester of pregnancy.
Cardiac monitoring of the fetus.
Ultrasound of the uterine scar every 7-10 days after 37 weeks of pregnancy.
The tactics of managing pregnant women with a well-to-do scar on the uterus does not differ from the generally accepted one.
An ultrasound scan is performed as early as possible. The main purpose of this study is to determine the place of attachment of the ovum in the uterus. If it is located in the isthmus on the anterior wall of the uterus (in the area of \u200b\u200bthe scar after cesarean section in the lower uterine segment), it is medically advisable to terminate the pregnancy, which is performed using a vacuum aspirator; since the proteolytic properties of the chorion, as pregnancy progresses, can lead to the inferiority of even a wealthy scar on the uterus, to presentation and ingrowth of the placenta into the scar, and to rupture of the uterus. The question of maintaining or terminating pregnancy is in the competence of the woman herself. With an uncomplicated course of pregnancy and the presence of a scar on the uterus, the next comprehensive examination is carried out at 37-38 weeks of gestation in a hospital where delivery of a pregnant woman is expected (level III obstetric hospitals).
Delivery of pregnant women with a scar on the uterus after cesarean section
The question of the method of delivery must be agreed with the pregnant woman. The task of the obstetrician is to explain in detail to her all the benefits and risks of both repeated cesarean section and spontaneous delivery. The final decision is made by the woman herself in the form of written informed consent to one of the delivery methods. In the absence of absolute indications for a planned caesarean section, preference should be given to childbirth through the vaginal birth canal, and, moreover, to their spontaneous onset.
Managing childbirth through the vaginal birth canal is permissible if a number of conditions are met:
- one history of cesarean section with a transverse incision in the uterus in the lower segment;
- the absence of extragenital diseases and obstetric complications, which served as indications for the first operation;
- the presence of a well-to-do scar on the uterus (based on the results of clinical and instrumental studies);
- localization of the placenta outside the uterine scar;
- cephalic presentation of the fetus;
- matching the size of the mother's pelvis and the fetal head;
- availability of conditions for emergency delivery by cesarean section: highly qualified medical personnel; the ability to perform a caesarean section on an emergency basis no later than 15 minutes after the decision on the operation is made.
Indications for repeated abdominal birth in the presence of a scar on the uterus after cesarean section:
- scar on the uterus after corporal cesarean section;
- an insolvent scar on the uterus for clinical and echoscopic signs;
- scar on the uterus after isthmus plasty;
- placenta previa in the scar;
- two or more scars on the uterus after cesarean sections in the lower uterine segment;
With a second cesarean section, a prerequisite is the excision of an inconsistent scar on the uterus, which significantly reduces the risk of complications during subsequent pregnancy.
Labor management in women with uterine scar after myomectomy
When choosing the method of delivery in women with a scar on the uterus after myomectomy, the decisive importance belongs to the nature, volume and method (laparotomic or laparoscopic) of the operation performed. The risk of rupture of the uterus along the scar after myomectomy during spontaneous labor is determined by the depth of the tumor in the myometrium.
Indications for cesarean section after myomectomy outside of pregnancy:
- a scar on the uterus after removal of the interstitial or subserous-interstitial nodes located on the posterior wall of the uterus;
- scar on the uterus after removal of cervical fibroids;
- scar on the uterus after removal of intraligamentary fibroids;
- scars on the uterus after removal of several large interstitial subserous nodes;
- burdened obstetric history;
- breech presentation of the fetus;
- FPN (fetoplacental insufficiency);
- the age of primipara is over 30 years old;
- scar after myomectomy performed by laparoscopic access.
When delivering pregnant women with a scar on the uterus after myomectomy outside of pregnancy and the absence of indications for caesarean section, spontaneous delivery is preferable.
A scar on the uterus after a myomectomy performed during pregnancy is an indication for a cesarean section.
Delivery of pregnant women with a scar on the uterus after reconstructive plastic surgery, uterine perforation and ectopic pregnancy
Indications for caesarean section:
- scar on the uterus after metroplasty (Strassmann's operation, removal of the rudimentary horn of the uterus with opening the uterine cavity, plastic isthmus for an insolvent scar on the uterus after cesarean section);
- a scar after perforation of the uterus, located in the isthmus along the back wall;
- a scar after removal of a cervical pregnancy, pregnancy in the rudimentary horn of the uterus, the stump of the previously removed tube.
After giving birth through the vaginal birth canal with a scar on the uterus, it is necessary to conduct a control manual examination of the walls of the uterine cavity.
Prevention of uterine scar failure
Creation of optimal conditions for the formation of a well-to-do scar on the uterus during operations on the uterus: suturing the incision on the uterus with separate muscle-muscular sutures or with a continuous suture (but not reverse) using synthetic absorbable suture threads (vicryl, monopril, etc.).
Prevention, timely diagnosis and adequate therapy of postoperative complications.
Objective assessment of the state of the scar on the uterus before pregnancy.
Source: wikimed.pro
Childbirth with a scar on the uterus ICD code 10
A scar (cicatrix) is a dense formation consisting of hyalinized connective tissue rich in collagen fibers, resulting from tissue regeneration when its integrity is violated.
A scar on the uterus is the area of \u200b\u200bthe uterus in which surgical interventions were performed [cesarean section (CSC)], myomectomy, reconstructive plastic surgery).
It should be noted that the concept of "scar on the uterus after a cesarean section", adopted in our country, is not entirely successful, since the scar is often not found during repeated surgery. Foreign authors usually use the terms "previous cesarean section" and "transferred myomectomy".
PO CODE ICD-10
O34.2 Postoperative uterine scar requiring maternal medical attention.
O75.7 Vaginal delivery following previous caesarean section
O71.0 Uterine rupture before labor begins.
O71.1 Uterine rupture during labor.
O71.7 Obstetric hematoma of the pelvis.
O71.8 Other specified obstetric injuries
O71.9 Obstetric injury, unspecified
According to various authors, a scar on the uterus after cesarean section is noted in 4–8% of pregnant women, and about 35% of abdominal births in the population are repeated. The prevalence of cesarean section in Russia has increased 3 times over the past decade and is 16%, and according to foreign authors, about 20% of all births in developed countries end with a cesarean section.
There are no statistical indicators of the number of pregnant women with a scar on the uterus after myomectomy and reconstructive plastic surgeries, but at present, due to the development of uterine fibroids at an earlier age, rapid growth tumors in women of reproductive age and its large size, preventing the onset and gestation of pregnancy, myomectomy was included in the complex of pregravid preparation. At the onset of pregnancy in women with uterine fibroids, obstetricians and gynecologists also perform myomectomy more often than 10-15 years ago. Thus, the number of pregnant women with uterine scar after myomectomy is constantly increasing.
Allocate a wealthy and inconsistent scar on the uterus. There is also a classification based on the cause of the uterine scar.
· A scar on the uterus after a cesarean section.
- In the lower uterine segment.
- Corporeal scar on the uterus.
- Isthmic-corporal scar on the uterus.
· Scar on the uterus after conservative myomectomy before and during pregnancy.
- Without opening the uterine cavity.
- With the opening of the uterine cavity.
- A scar on the uterus after removal of the subserous-interstitial node.
- Scar on the uterus after removal of intraligamentary fibroids.
· A scar on the uterus after perforation of the uterus [with intrauterine interventions (abortion, hysteroscopy)].
· A scar on the uterus after an ectopic pregnancy, located in the interstitial section of the fallopian tube, at the place where the rudimentary horn of the uterus communicates with the main uterine cavity, in the cervix after removal of the cervical pregnancy.
· Scar on the uterus after reconstructive surgery (Strassmann's operation, removal of the rudimentary horn of the uterus).
A scar on the uterus is formed after cesarean section, conservative myomectomy, uterine perforation, tubectomy, etc.
Scarring is a biological mechanism for the healing of damaged tissues. Healing of the dissected uterine wall can occur through both restitution (full regeneration) and substitution (defective regeneration). With full-fledged regeneration, wound healing occurs due to smooth muscle cells (myocytes), with substitution - bundles of coarse fibrous connective, often hyalinized tissue.
CLINICAL PICTURE OF UTERINE RUPTURE ACROSS THE SCAR
Ruptures of the uterus with dystrophic changes in the myometrium or the presence of scar tissue occur without a pronounced clinical picture (incorrectly named "asymptomatic"). Despite the erased and unexpressed nature of the disease, the symptoms do occur and you need to know them.
In the presence of a postoperative scar on the uterus, ruptures can occur both during pregnancy and during childbirth.
By clinical course the same stages are distinguished as in the case of a mechanical one - a threatening, begun and completed rupture of the uterus.
Symptoms of a ruptured uterus along the scar during pregnancy
Symptoms of a threatening rupture of the uterus along the scar during pregnancy are due to reflex irritation of the uterine wall in the area of \u200b\u200bexpanding scar tissue:
·nausea;
Vomiting;
Pain:
- in the epigastric region, followed by localization in the lower abdomen, sometimes more on the right (imitate the symptoms of appendicitis),
- in the lumbar region (imitate renal colic);
Soreness, sometimes local, in the area of \u200b\u200bthe postoperative scar on palpation, where it is felt
deepening.
Symptoms of the onset of rupture of the uterus along the scar during pregnancy are determined by the presence of a hematoma in the wall of the uterus due to the appearance of a rupture of its wall and blood vessels. The symptoms of a threatening rupture are joined by:
· Hypertonicity of the uterus;
· Signs of acute fetal hypoxia;
· Possible bleeding from the genital tract.
Symptoms of a completed uterine rupture during pregnancy: to the clinical picture of a threatening and
of the beginning of ruptures, symptoms of pain and hemorrhagic shock are attached:
Worsens general state and well-being;
Weakness, dizziness appears, which may initially be of reflex genesis, and subsequently
be conditioned by blood loss;
· Obvious symptoms of intra-abdominal bleeding and hemorrhagic shock - tachycardia, hypotension, pallor of the skin.
When a rupture occurs in the scar tissue, deprived of a large number of vessels, bleeding into the abdominal cavity can be moderate or insignificant. In such cases, the symptoms associated with acute fetal hypoxia come to the fore.
Rupture of the uterus along the scar during labor
Ruptures of the uterus along the scar during labor occur in the presence of postoperative scars on the uterus or dystrophic changes in it, in multiparous.
Threatening uterine rupture during labor is characterized by the following symptoms:
·nausea;
Vomiting;
Epigastric pain;
Various variants of violation of the contractile activity of the uterus - discoordination or weakness of labor, especially after the outflow of amniotic fluid;
· Painful contractions, not corresponding to their strength;
• restless behavior of the woman in labor, combined with weak labor activity;
· Delay in the advancement of the fetus with full dilatation of the cervix.
When the rupture of the uterus begins along the scar in the first stage of labor due to the presence of a hematoma in the wall of the uterus:
· Constant, not relaxing tension of the uterus (hypertonicity);
Pain on palpation in the lower segment or in the area of \u200b\u200bthe alleged scar, if any;
· Signs of fetal hypoxia;
· Bleeding from the genital tract.
In most women in labor, the time interval from the onset of symptoms of an incipient rupture to the moment
accomplished is calculated in minutes.
The clinic of the completed rupture of the uterus along the scar is similar to that observed during pregnancy - these are mainly signs of hemorrhagic shock and antenatal fetal death.
In vaginal examination, it is characteristic to determine a high-standing movable head, previously pressed or firmly standing at the entrance to the pelvis.
If the rupture of the uterus along the scar occurs in the II stage of labor, then the symptoms are not clearly expressed:
· Weak, but painful attempts, gradually weakening until they stop;
• pain in the lower abdomen, sacrum;
· Bleeding from the vagina;
· Acute hypoxia of the fetus with its possible death.
Sometimes the rupture of the uterus along the scar occurs with the last push. At the same time, it can be very difficult to diagnose a gap. A child is born spontaneously, alive, without asphyxiation. The placenta is independently separated, the placenta is born, and only later the symptoms associated with hemorrhagic shock gradually increase, seemingly "causeless" hypotension, sometimes epigastric pain. To clarify the diagnosis is possible only with a manual examination of the uterus or with laparoscopy.
Incomplete uterine rupture can occur at any stage of labor.
Diagnosis of pregnancy complications in women with a uterine scar is based on a thorough history, physical examination, and laboratory data.
Thorough collection of anamnesis should include obtaining information about a previous caesarean section (indications), time of the COP, the presence of spontaneous childbirth before and after surgery, the number of pregnancies between the operation and a real pregnancy, their results (abortion, miscarriage, non-developing pregnancy), about the presence of living children, cases of stillbirth and death of children after previous births, about the course of this pregnancy.
It is necessary to palpate the scar on the anterior abdominal wall and on the uterus, measure the size of the pelvis and determine the estimated weight of the fetus. At 38–39 weeks of gestation, the readiness of the pregnant woman's body for childbirth is assessed.
·General blood analysis.
·General urine analysis.
· Biochemical blood test (determination of the concentration of total protein, albumin, urea, creatinine, residual nitrogen, glucose, electrolytes, direct and indirect bilirubin, activity of alanine aminotransferase, aspartate aminotransferase and alkaline phosphatase).
· Coagulogram, hemostasiogram.
· Hormonal status of FPK (concentration of placental lactogen, progesterone, estriol, cortisol) and assessment of the content of a-fetoprotein.
· Ultrasound of the fetus with dopplerometry of the vessels of the umbilical cord, fetal aorta, middle cerebral artery of the fetus and placenta is shown from the end of the second trimester of pregnancy.
· Cardiac monitoring of the fetus.
· Ultrasound of the scar on the uterus every 7-10 days.
DIAGNOSTICS OF THE STATE OF THE SCAR ON THE UTERINE OUT OF PREGNANCY
All women with a scar on the uterus after a cesarean section should be registered immediately after discharge from the hospital. The main purpose of dispensary observation is early diagnosis and treatment of late complications of surgery (genital fistulas, tubo-ovarian formations) and prevention of pregnancy during the first year after surgery. During lactation, for the purpose of hormonal contraception, linestrenol (gestagen) is used, which does not provide negative influence on a newborn. After the end of lactation, estrogen-gestagenic contraceptives are prescribed.
In the complex of measures to prepare for the next pregnancy, an important role is played by the assessment of the condition of the scar on the uterus. Hysterography, hysteroscopy and ultrasound examination (ultrasound) are considered informative methods for determining the state of the scar on the uterus in a non-pregnant woman.
· Hysterography is performed on the 7th or 8th day of the menstrual cycle (but not earlier than 6 months after the operation) in frontal and lateral projections. Using this method, you can study changes in the inner surface of the postoperative scar on the uterus. Allocate following signs inconsistency of the postoperative scar: a change in the position of the uterus in the small pelvis (significant displacement of the uterus anteriorly), jagged and thinned contours of the inner surface of the uterus in the area of \u200b\u200bthe alleged scar, "niches" and filling defects.
· Hysteroscopy is done on the 4th or 5th day of the menstrual cycle, when the functional layer of the endometrium is completely rejected, and the underlying tissue is visible through the thin basal layer. In case of scar failure, retraction or thickening in the area of \u200b\u200bthe scar is usually noted. The whitish color of the scar tissue, the absence of blood vessels indicate a pronounced predominance of the connective tissue component, and retraction - about the thinning of the myometrium as a result of defective regeneration. The prognosis for gestation and delivery through the vaginal birth canal is contradictory. An unvisualized uterine scar and a scar with a predominance of muscle tissue serve as a sign of its anatomical and morphological usefulness. These women may become pregnant 1-2 years after surgery.
· Ultrasound signs of scar failure on the uterus include an uneven contour along the back wall of a filled bladder, thinning of the myometrium, discontinuity of the scar contours, a significant number of hyperechoic inclusions (connective tissue). With two-dimensional ultrasound, pathological changes in the area of \u200b\u200bthe scar on the uterus are found much less often than with hysteroscopy (in 56 and 85% of cases, respectively). However, thanks to Doppler and three-dimensional reconstruction, which can be used to assess hemodynamics in the scar (development of the vasculature), the information content of ultrasound assessment of the state of the scar on the uterus has increased significantly.
The results obtained from additional methods for diagnosing the state of a scar on the uterus outside of pregnancy are entered into an outpatient card and taken into account when deciding on the possibility of planning a subsequent pregnancy.
A differential diagnosis is required between the true threat of termination of pregnancy and the presence of an inconsistent scar on the uterus (Table 52-6). It is also necessary to carry out a differential diagnosis. acute appendicitis and renal colic. Clarification of the diagnosis is carried out in a hospital setting on the basis of clinical symptoms, ultrasound data, and the effect of therapy. If there is an inconsistent scar on the uterus, the pregnant woman should be in the hospital until delivery. In this case, a clinical assessment of the condition of the pregnant woman, the fetus and the scar on the uterus is carried out daily. The ultrasound is repeated every week. With an increase in clinical or ultrasound symptoms of inconsistency of the scar on the uterus, operative delivery is indicated for vital indications on the part of the mother, regardless of the duration of pregnancy.
Table 52-6. Differential diagnosis threats of termination of pregnancy and inconsistency of the scar on the uterus after cesarean section in the lower uterine segment
INDICATIONS FOR CONSULTING OTHER SPECIALISTS
Consultation with an anesthesiologist is indicated if it is necessary to provide anesthetic support for operative delivery or for the purpose of pain relief during labor.
Pregnancy 32 weeks Head presentation of the fetus. Inconsistent scar on the uterus after cesarean section in 2002. Dropsy of pregnant women. Anemia of the 1st degree.
Pregnancy 38 weeks Head presentation of the fetus. A scar on the uterus after a cesarean section in 2006. Placental insufficiency. ZRP I degree. Combined preeclampsia of moderate severity 8 points against the background of arterial hypertension.
Pregnancy 37 weeks Scars on the uterus after myomectomy and small cesarean section in 2000. Elderly primiparous.
Pregnancy 36 weeks Breech presentation of the fetus. Scar on the uterus after corporal cesarean section in 1999. Anemia.
COMPLICATIONS OF GESTATION IN THE PRESENCE OF A SCAR ON THE UTERUS
The course of pregnancy in the presence of a scar on the uterus after a cesarean section has a number of clinical features... These patients often have a low location or previa of the placenta, its true rotation, incorrect position of the fetus, and when the placenta is localized in the area of \u200b\u200bthe scar on the uterus, PN often develops.
One of the most frequent complications of the gestation process in pregnant women with a scar on the uterus is the threat of termination of pregnancy. Symptoms of threatened termination in the first trimester of pregnancy have no etiological connection with the presence of a scar on the uterus. Conservation therapy is prescribed according to the established diagnosis (insufficient synthesis of progesterone, hyperandrogenism, APS, etc.). Treatment on an outpatient basis is possible, however, if there is no effect, hospitalization is necessary to clarify the diagnosis and correct the therapy. When isthmic-cervical insufficiency is detected, surgical correction of this pathology in this contingent of patients is not indicated, since the presence of a scar on the uterus in combination with the threat of termination of pregnancy can lead to rupture of the uterus along the scar. Treatment of this complication includes antispasmodic therapy, administration of magnesium sulfate, bed rest, and the use of an unloading vaginal pessary. Treatment of other complications of pregnancy in women with an operated uterus does not fundamentally differ from the generally accepted one.
MANAGEMENT OF PREGNANT WOMEN WITH A SCAR ON THE UTERINE
During pregnancy (in the first trimester), a general examination is carried out, and, if necessary, consultations of related specialists. Be sure to appoint an ultrasound, the main purpose of which is to determine the place of attachment of the ovum in the uterus. If it is located in the isthmus on the anterior wall of the uterus (in the area of \u200b\u200bthe scar after cesarean section in the lower uterine segment), it is advisable to terminate the pregnancy, which is performed using a vacuum aspirator. This tactic is due to the fact that the proteolytic properties of the chorion, as pregnancy progresses, can lead to the inferiority of even a wealthy scar on the uterus and its rupture, and the outcome of this pregnancy is only a repeated cesarean section. However, there are no absolute contraindications to prolonging pregnancy in this case, and the woman herself decides whether to terminate the pregnancy. The next screening examination, including ultrasound and the study of the hormonal status of the fetoplacental complex (FPK), is carried out at 20-22 weeks of gestation and its purpose is to diagnose fetal malformations, whether its size matches the gestational age, signs of placental insufficiency (PN), especially when the placenta is located in the area of \u200b\u200bthe scar. For the treatment of PN, hospitalization is indicated. With an uncomplicated course of pregnancy and a well-to-do scar on the uterus, the next comprehensive examination is carried out at 37–38 weeks of gestation in a hospital, where it is expected to deliver the pregnant woman.
In childbirth, antispasmodic, sedative and antihypoxic drugs must be used, medicinesthat improve uteroplacental blood flow.
DELIVERY OF PREGNANT WOMEN WITH A SCAR ON THE UTERINE
Delivery of pregnant women with a scar on the uterus after cesarean section
Most obstetricians have a basic postulate when delivering pregnant women with a scar on the uterus after a cesarean section: one cesarean section is always a cesarean section. However, both in our country and abroad, it has been proven that in 50–80% of pregnant women with an operated uterus, vaginal birth is not only possible, but also preferable. The risk of a repeat cesarean section, especially for the mother, is higher than the risk of a spontaneous birth.
Spontaneous childbirth in pregnant women with a scar on the uterus after cesarean section
Managing labor through the vaginal birth canal in the presence of a scar on the uterus after a cesarean section is permissible under a number of conditions.
· One previous cesarean section with a transverse incision in the uterus in the lower segment.
· Absence of extragenital diseases and obstetric complications, which served as indications for the first operation.
· Consistency of the scar on the uterus (according to the results of clinical and instrumental studies).
· Localization of the placenta outside the uterine scar.
· Head presentation of the fetus.
· Matching the size of the mother's pelvis and the fetal head.
· Availability of conditions for emergency delivery by caesarean section (highly qualified medical personnel, the possibility of performing a caesarean section on an emergency basis no later than 15 minutes after the decision on the operation is made).
The question of the method of delivery must be agreed with the pregnant woman. The obstetrician should explain in detail to her all the benefits and risks of both repeated cesarean section and vaginal delivery. The final decision should be made by the woman herself in the form of written informed consent to one of the methods of delivery. In the absence of absolute indications for a planned caesarean section, preference should be given to childbirth through the vaginal birth canal, moreover, with their spontaneous onset.
Childbirth in the presence of a scar on the uterus, as a rule, proceeds according to the standard mechanism characteristic of primiparous or multiparous. The most frequent complications of childbirth in women with a scar on the uterus are untimely rupture of amniotic fluid, abnormalities of labor (which should be considered as a threat of uterine rupture), clinical discrepancy between the size of the mother's pelvis and the fetal head (due to more frequent than in the population, the location of the fetal head in posterior form), the appearance of signs of threatening rupture of the uterus. During childbirth, continuous cardiac monitoring of the fetus is necessary, with clinical assessment the nature of labor and the state of the scar on the uterus. Childbirth should be carried out with an expanded operating room, with an infusion system connected. In addition to the clinical (palpation) assessment of the state of the scar on the uterus in the process of spontaneous delivery, ultrasound can be used, with the help of which, in addition to assessing the condition of the scar on the uterus in the first stage of labor, the type and position of the fetus, the location of the fetal head in relation to the planes of the small pelvis of the woman in labor, are specified (ultrasound registration of the opening of the uterine pharynx), due to which the number of vaginal examinations is reduced, which is useful in preventing infectious complications in women in labor with a high probability of operative delivery.
Labor pain relief in women with a scar on the uterus is carried out according to generally accepted rules, including the use of epidural analgesia. The method of anesthesia during childbirth depends on the nature of the extragenital or other obstetric pathology.
A scar on the uterus after a cesarean section is not considered a contraindication to the use of other obstetric and anesthetic aids in childbirth, such as labor induction or rhodostimulation. With a prolonged II stage of labor or the onset of fetal hypoxia, delivery must be accelerated by dissecting the perineum. With acute hypoxia of the fetus and the head located in a narrow part of the pelvic cavity, labor can be completed by applying obstetric forceps or a vacuum extractor.
Manual examination of the uterus immediately after childbirth is considered mandatory in the absence of ultrasound control.
Symptoms of uterine rupture may appear long after delivery, therefore, it is advisable to repeat ultrasound 2 hours after delivery in order to diagnose dissecting retrovesical hematomas, which are the result of undiagnosed uterine rupture.
Indications for a cesarean section in the presence of a scar on the uterus after a cesarean section:
· Scar on the uterus after corporal caesarean section.
· Inconsistent scar on the uterus for clinical and ultrasound signs.
· Placenta previa.
· Two or more scars on the uterus after cesarean sections.
· A woman's categorical refusal to give birth through the natural birth canal.
Labor management in women with uterine scar after myomectomy
When choosing a method of delivery in women with a scar on the uterus after myomectomy, the nature and volume of the operation performed are of decisive importance. The incidence of inconsistent scars after myomectomy reaches 21.3%. The risk of rupture of the uterus along the scar after myomectomy during spontaneous delivery depends on the depth of the tumor in the myometrium (interstitial, subserous-interstitial, subserous or submucous myoma) before surgery, the technique of surgery, localization of the scar on the uterus. Indications for operative delivery are absolute and relative. The absolute indications for caesarean section after myomectomy outside of pregnancy are given below.
· A scar on the uterus after removal of an interstitial or subserous-interstitial node located on the posterior wall of the uterus.
· Scar on the uterus after removal of intraligamentary fibroids.
· Scars on the uterus after removal of several large interstitial-subserous nodes.
When delivering pregnant women with a scar on the uterus after myomectomy outside of pregnancy and the absence of absolute indications for cesarean section, it is preferable to carry out labor through the vaginal birth canal. In the presence of a burdened obstetric history, post-term pregnancy, breech presentation of the fetus, PN, primiparous age over 30 years, indications for cesarean section after myomectomy are expanded.
A scar on the uterus after a myomectomy performed during pregnancy is an indication for a cesarean section.
Labor management in women with a scar on the uterus after reconstructive plastic surgery
· After metroplasty, preference should be given to caesarean section in order to prevent maternal injury during spontaneous childbirth.
· After removal of the rudimentary horn of the uterus without opening its main cavity, birth through the vaginal birth canal is possible.
Labor management in women with a scar on the uterus after uterine perforation
Childbirth after uterine perforation during intrauterine interventions is a difficult and responsible task. The location of the perforation in relation to the walls of the uterus is of great importance. The location of the scar in the isthmus and on the posterior wall of the uterus is considered unfavorable. During such delivery, uterine ruptures, hypotonic bleeding, pathology of placenta separation are possible, especially in women with a complicated course of the operation itself and the postoperative period.
The obstetric prognosis is more favorable in cases where the scar is located on the anterior wall of the uterus, and the operation was limited only to suturing the perforation without additional dissection of the uterine wall. In the absence of complicating circumstances, birth through the vaginal birth canal is possible, followed by a control manual examination of the walls of the uterine cavity.
Labor management in women with uterine scar after ectopic pregnancy
The choice of delivery method after an ectopic pregnancy depends on the volume of the operation and the woman's age. Surgical interventions for cervical pregnancy, pregnancy in the rudimentary uterine horn (if it has a message with the main cavity), the interstitial part of the fallopian tube, the stump of the removed early tube serve as an indication for a cesarean section.
PREDICTION AND PREVENTION OF GESTION COMPLICATIONS
Pregnant women with a scar on the uterus are considered a risk group for the development of the following obstetric and perinatal complications: spontaneous abortion, rupture of the uterus along the scar, premature birth, PN, hypoxia and intrauterine fetal death, birth trauma of the mother and fetus, high maternal and perinatal mortality. To prevent these complications, careful dispensary observation for a pregnant woman, timely detection of complications and their treatment in multidisciplinary obstetric hospitals. Prevention of complications is based on the widespread promotion of pre-conceptional preparation of women with a scar on the uterus, which includes the following activities.
· Communication of the risk associated with the presence of a scar on the uterus.
- Risk for the mother: rupture of the uterus along the scar, bleeding, maternal mortality, purulent-septic complications; miscarriage.
- Risk to the fetus and newborn: prematurity, birth trauma, neonatal complications of varying severity.
· Diagnosis and treatment of concomitant gynecological and extragenital diseases before pregnancy.
· Screening for sexually transmitted infections (STIs) and sanitation of foci of infection.
TREATMENT OF COMPLICATIONS DURING LABOR AND POSTNATAL PERIOD
The most formidable complication in childbirth is rupture of the uterus along the scar. When conducting labor through the vaginal birth canal in women with a scar on the uterus, overdiagnosis of uterine rupture should be preferred, rather than underestimating such a serious complication. It is considered extremely difficult to assess the first symptoms of the onset of rupture of the uterus along the scar. Diagnosis of uterine rupture is carried out taking into account the clinical picture: pain in the epigastric region, nausea, vomiting, tachycardia, local soreness, bleeding from the genital tract, shock, etc. Signs of deterioration of the fetus, weakening of the contractile activity of the uterus can be symptoms of an incipient rupture, and often first. Additional diagnostic methods (ultrasound, tococardiography) are invaluable in childbirth.
Distinguish between complete rupture and incomplete rupture of the uterus (stratification, scar spreading), when the peritoneum remains intact. Tactics for a ruptured uterus is an emergency caesarean section. The volume of surgical intervention depends on the extent of the injury: when the uterus ruptures, only in the area of \u200b\u200bthe scar after the fetus is removed, the scar is excised and sutured, and when the uterus is ruptured, complicated by the formation of intraligamentary hematomas, it is extirpated. With subsequent pregnancy, operative delivery is indicated.
Indications for cesarean section in childbirth are expanded with negative dynamics of the fetus, the appearance clinical signs threatening rupture of the uterus, the absence of conditions for the careful spontaneous completion of labor.
PREVENTION OF UTERINE RUPTURE ACROSS THE SCAR
Prevention of rupture of the uterus along the scar consists in carrying out the following measures.
Creation of optimal conditions for the formation of a wealthy scar on the uterus during the first cesarean section (incision on the uterus according to Derfler) and other operations on the uterus: suturing the incision on the uterus with separate musculoskeletal sutures using synthetic absorbable suture threads (vicryl, monopril, etc.) ...
· Prediction, prevention, timely diagnosis and adequate therapy of postoperative complications.
· Objective assessment of the state of the scar on the uterus before pregnancy and during gestation.
· Screening examination during pregnancy.
· Careful selection of pregnant women for vaginal delivery.
· Thorough cardiotocographic and ultrasound control during spontaneous labor.
· Adequate pain relief during spontaneous labor.
· Timely diagnosis of threatening and / or incipient rupture of the uterus.
Infiltration after surgery is one of the most common complications after surgery. It can develop after any operation - if you had an appendicitis cut out, a hernia removed, or even just an injection was given.
Therefore, it is important to very carefully monitor your condition after surgery. It is quite simple to cure such a complication if it is diagnosed in time. But if you tighten it, it can develop into an abscess, and this is already fraught with a breakthrough of the abscess and blood poisoning.
What it is?
The term itself is a fusion of two Latin words: in - "in" and filtratus - "filtered". Doctors call this word a pathological process, when particles of cells (including blood numbers), blood itself, lymph accumulate inside tissues or any organ. Outwardly, it looks like a dense formation, but simply a tumor.
There are 2 main forms of this phenomenon - inflammatory (this is usually the complication after surgery) and tumor. Inside the second formation, there is not innocent blood and lymph, but tumor cells, and very often - cancer cells. Sometimes doctors call an infiltrate a site on the body, where an anesthetic, antibiotic or other substances are injected during treatment. This type is called "surgical".
The inflammatory process can begin even before the operation. Especially often, appendicular infiltrate is diagnosed, which develops almost in parallel with inflammation of the appendix. It is even more common than a complication after appendicitis surgery. Another "popular" option is a swelling in the mouth of children, the reason is fibrous pulpitis.
Varieties
Inflammatory infiltration is the main type of such pathology, which often appears after surgery. There are several types of such inflammation, depending on which cells inside the tumor are the most.
- Purulent (polymorphonuclear leukocytes have collected inside).
- Hemorrhagic (erythrocytes).
- Round cell, or lymphoid (lymphoid cells).
- Histiocytic-plasma cell (inside the plasma elements and histiocytes).
Inflammation of any nature can develop in several directions - or dissolve over time (in 1-2 months), or turn into an ugly scar, or develop into an abscess.
Scientists consider the infiltrate of the postoperative suture to be a special type of inflammatory. This disease is especially insidious - it can "pop out" and a week or two after the operation, and after 2 years. The second option happens, for example, after a cesarean section, and the risk that the inflammation will develop into an abscess is quite high.
Causes
No one is immune from the appearance of purulent, hemorrhagic and other formations after surgery. Complication occurs in young children and in adult patients, after a banal appendicitis and after surgery to remove the uterus (paracervical and other tumors).
Experts name 3 main reasons for this phenomenon - trauma, odontogenic infections (in the oral cavity) and other infectious processes. If you come to the doctor because the postoperative suture has become inflamed, a number of other reasons are added:
- an infection has entered the wound;
- postoperative drainage was incorrectly performed (usually in overweight patients);
- through the fault of the surgeon, the layer of subcutaneous fat was damaged, and a hematoma appeared;
- suture material has high tissue reactivity.
If the scar becomes inflamed only a few months or years after surgery, the suture material is to blame. This pathology is called ligature (a ligature is a dressing thread).
A propensity to allergies in a patient can also provoke pathology, weak immunity, chronic infections, congenital diseases, etc.
Symptoms
The postoperative complication does not develop immediately - usually on the 4-6th day after the X hour (surgical intervention). Sometimes even later - after one and a half to two weeks. The main signs of incipient inflammation in the wound are:
- subfebrile temperature (it rises by only a few divisions, but it is impossible to bring it down);
- when pressing on the inflamed area, pain is felt;
- if you press very hard, a shallow fossa appears, which gradually straightens;
- the skin in the affected area swells and turns red.
If swelling occurs after surgery to remove an inguinal hernia, other symptoms may be added. About the pathological accumulation of cells in the abdominal cavity will say:
- aching pain in the peritoneal region;
- bowel problems (constipation);
- hyperemia (strong blood flow to sore spots).
With hyperemia, edema occurs and boils pop out, heart rate increases, the patient suffers from headaches.
What is post-injection infiltrate?
Infiltration after injection is one of the most common complications after injection, along with hematomas. It looks like a small dense bump in the place where the needle with the medicine was stuck. The predisposition to such a mini-complication is usually individual: someone has a seal on the skin after each injection, and someone has never encountered such a problem in their entire life.
The following reasons can provoke a similar reaction of the body to a banal injection:
- the nurse performed poorly on the antiseptic treatment;
- the needle on the syringe is too short or blunt;
- the wrong place for the injection was chosen;
- injections are done constantly in the same place;
- the medicine is being administered too quickly.
Such a sore can be cured with conventional physiotherapy, iodine mesh or compresses with diluted Dimexide. Will help and folk methods: cabbage leaves, aloe, burdock compresses. For greater effectiveness, before compressing, you can lubricate the lump with honey.
Diagnostics
It is usually not difficult to diagnose such postoperative pathology. When making a diagnosis, the doctor relies primarily on the symptoms: temperature (what and how long it lasts), the nature and intensity of pain, etc.
Most often, the tumor is determined by palpation - it is a dense formation with uneven and indistinct edges, which responds with pain when palpated. But if the surgical manipulations were carried out on the abdominal cavity, then the seal can hide deep inside. And with a finger examination, the doctor simply will not find him.
In this case, more informative diagnostic methods come to the rescue - ultrasound and computed tomography.
Another mandatory diagnostic procedure is a biopsy. Tissue analysis will help to understand the nature of inflammation, find out which cells have accumulated inside, establish whether there are malignant cells among them. This will allow you to find out the cause of the problem and correctly draw up a treatment regimen.
Treatment
The main goal in the treatment of postoperative infiltrate is to relieve inflammation and prevent the development of an abscess. To do this, you need to restore blood flow in a sore spot, relieve swelling and eliminate pain. First of all, conservative therapy is used:
- Antibiotic treatment (if the infection is caused by bacteria).
- Symptomatic therapy.
- Local hypothermia (artificial decrease in body temperature).
- Physiotherapy.
- Bed rest.
Effective procedures are considered to be UV irradiation of the wound, laser therapy, mud therapy, etc. The only contraindication for physiotherapy is purulent inflammation. In this case, warming up and other procedures will only accelerate the spread of the infection and may cause an abscess.
When the first signs of an abscess appear, a minimally invasive intervention is first used - drainage of the affected area (under ultrasound control). In the most difficult cases, the abscess is opened in the usual way, using laparoscopy or laparotomy.
Treatment of a postoperative suture with complications is also traditionally carried out using conservative methods: antibiotics, novocaine blockade, physiotherapy. If the tumor has not resolved, the suture is opened, cleaned and sutured again.
An infiltrate after surgery can form in a patient of any age and health condition. By itself, this tumor usually does not carry any harm, but it can serve as the initial stage of an abscess - a severe purulent inflammation. The danger is that sometimes pathology develops several years after a visit to the operating room, when the scar becomes inflamed. Therefore, it is necessary to know all the signs of such a disease and, at the slightest suspicion, consult a doctor. This will help avoid new complications and additional surgical interventions.
Article for the site "Recipes for health" prepared by Nadezhda Zhukova.
* By clicking on the "Submit" button I agree with
Source: zdorovieiuspex.ru