Differential diagnosis of diabetic nephropathy. Treatment of complications for diabetes mellitus - kidney nephropathy. Forecast and prevention of diabetic nephropathy
Around the world, diabetic nephropathy (DN) and developed due to her renal failure are the leading cause of patient mortality sugar diabetes (SD) type 1. In patients with SD 2 type of DN stands on a 2nd place among the causes of mortality after cardiovascular diseases.
Considering the widespread prevalence of SD, the continuous increase in the incidence of SD, as well as an increase in the life expectancy of patients with SD, a significant increase in the prevalence of DN is predicted. In developed countries from 20 to 50% of the total number of deployment of renal renumber therapy (CPT) are patients with diabetes. In Russia, SD, as the cause of terminal renal failure (TPN), is 11.3% of all cases of renal renal failure (ZPN), which can be explained by a number of reasons: a shortage of dialysis places, a low lifetime in a population and high cardiovascular mortality.
The main purpose of the treatment of the developed DN is the warning of the development of TPN and a reduction in cardiovascular risks.
Therapeutic measures should affect the main pathogenetic mechanisms and risk factors affecting the development and progression of the DN; The greatest efficiency in the deceleration of the progression of the bottom can be achieved in a multifactoric approach (2C).
The basic principles of treatment of the day are corrected carbohydrate exchange, arterial pressure (Hell), lipid metabolism. As already mentioned, achieving optimal compensation of glycemia (HBA1C< 7%) имеет ведущее значение на стадии микроальбуминурии, тогда как на стадии протеинурии более значимым становится нормализация АД.
At the later stages of kidney damage, the need for anemia and phosphorous calcium exchange is joined. Starting from the microalbuminuria stage, special attention is paid to respect for the renal diet.
Features of the renal diet
Most researchers tend to the appropriateness of limiting protein consumption to 1.0 g / kg / day at DN at the microalbuminuria stage, chronic disease kidney (HBP) 1-3 stages; up to 0.8 g / kg / day with proteinuria, HBP 1-4 stage. It is advisable to partially replace animal proteins vegetable. The purpose of such restrictions is to reduce the hemodynamic burden on the kidneys and a decrease in the filtration load protein on the kidneys.
Low-facane diet is contraindicated with sharp infectious diseases, children's and adolescent period, pregnancy.
In the case of attaching arterial hypertension, an important treatment factor is the restriction of the cook salt. For patients with SD, this recommendation is particularly effective, since these patients are characterized by high solubleness. According to the latter European recommendations Samp patients even with normal blood pressure should limit the use of salt up to 5-6 g / day (it should be remembered that 1 teaspoon contains 5 g of cook salt). With increasing blood pressure, the restriction should be more stringent (up to 3 grams per day), which involves cooking from natural products without acceleration.
When reducing the kidney function, it is important to control the use of potassium food (no more than 2.4 g / day) and phosphates (0.8-1.0 g / day) and sufficient consumption of calcium due to products with its high content.
Refusal of tobaccoing is one of the necessary moments of changing the style of the patient's lifetime, since it is definitely shown that this harmful habit is associated with the risk of developing DN, and with its accelerated progression.
Reducing body weight is necessary with BMI\u003e 27 kg / m2.
Long-term control of glycemia at the HBA1C level is less than 7% is able to prevent and slow down the progression of the HBS in patients with SD. (1A).
It is allowed to maintain HBA1C more than 7% for patients having a high risk of hypoglycemia (1b) and patients with related cardiovascular diseases and limited expected lifelong lifespan (2C).
It is shown that in patients with microalbuminuria, which have not been achieved by the optimal control of glycemia, in 5-8 years old developing pronounced proteinuria and arterial hypertension. In patients who have microalbuminuria there were less than 100 mg / day, intensive insulin therapy led to a decrease in the excretion of albumin with urine to normal values.
Despite the assumptions of most authors, that at the stage of proteinuria, pathological mechanisms in the kidneys occur already regardless of the quality of compensation for carbohydrate exchanges, nevertheless control of glycemia and at the stage of proteinuria continues to play an important role in the progression of DN. Thus, the results of the study in patients with a kidney lesion, who suffered a pancreatic transplantation, showed that after 10 years after transplantation and persistent maintenance of normoglycemia, the reverse development of kidney structural changes was observed, confirmed by kidney biopsy data.
The normalization of carbohydrate exchange is ensured when choosing an intensified insulin-therapy regime, which mimics the physiological secretion of insulin healthy people: Introduction short insulin Before each intake of food and insulin of extended action one or twice a day.
It should be remembered that in contrast to endogenous exogenous insulin is excreted by the kidneys. With a decrease in the speed of glomeri filtration (SCF) to 20 ml / min, there is a decrease in insulin filtering and an increase in its half-life. This phenomenon requires a decrease. daily dose Insulin by 25% with a decrease in SCF from 50 to 10 ml / min and 50% at SCF less than 10 ml / min.
In the treatment of patients with SD 2 type with diabetic nephropathy, oral sugar-based drugs must be taken into account their pharmacodynamic features and removal paths.
Thus, patients with long-term flow of SD 2 and kidney pathology requires revision and correction of sugar therapy. Biguanide preparations are contraindicated in renal failure due to the risk of lactate-acidosis; Tiazolindions (Pioglitazone) Despite the safe pharmacokinetic profile, are not recommended for kidney pathology, since they have side effects In the form of a fluid delay, the development of heart failure. Such preparations from the sulfonylurea group as glibenklamide, glymepiride is not recommended for patients with renal failure Due to the risk of the development of hypoglycemic states.
In patients with diabetes of type 2 and renal failure, glyclaside, glycovidone and repaglinides can be used without a dose correction in the event that these patients have satisfactory glycemic control. Otherwise, the translation into insulin therapy is required.
Glyclaside provides low risk of hypoglycemic episodes and nephroprotective effect, which is confirmed in randomized clinical Research Advance, completed in 2008, which showed a significant decrease in the risk of TPN by 65%, the development or progression of the DN by 21% and macrollibuminuria by 30% in the group of intensive control of glycemia (HBA1C 6.5%) of the modified release glyclaside. An additional analysis of these studies submitted to the Congress of the European Association of Endocrinologists in 2010 showed that the intensive control of glycemia allowed not only to significantly reduce the risk of proteinuria's development, but also to ensure the regression of the day in 57% of patients.
Recommendations for the correction of arterial hypertension and control of Albuminuria
- The target level of systolic blood pressure in patients with SD is<140 мм рт.ст. (2В)
- The target level of diastolic blood pressure in patients with SD is<85 мм рт.ст. (целевой уровень 80-90 мм рт.ст.) (1А)
- Lower systolic blood pressure (<130 мм рт.ст.) могут рассматриваться у пациентов с явной протеинурией, у которых польза от ренопротективного эффекта перевешивает потенциальные риски (более молодые с высокой протеинурией/альбуминурией) при условии мониторирования динамики СКФ (2В)
- Antihypertensive therapy should be individualized, and reduction of systolic blood pressure<120 мм рт.ст. и диастолического АД <70 мм рт.ст. следует избегать (2В)
- Preparations of selection in the treatment of AG with any stage of the day are the means of blocking renin-angiotensin-aldosterone system (RAAS): inhibitors of angiotensin glossy enzyme (IAPF) and angiotensin receptor blockers (Branch) (1A)
- With the intolerance to the IAPF and the sconce of interchangeable.
- The second line of hypotensive therapy is saluretics, block places of slow calcium channels (BKK), renin inhibitors; Beta blockers, A-blockers and central drugs should be considered as the last steps of AG therapy.
- Patients with excretion of albumin over 30 mg / day Recommended by the use of IAPF or Branch (1A)
- ACE inhibitor or sconium is not recommended for primary prevention of diabetic nephropathy in patients with diabetes mellitus with normal arterial pressure and excretion of albumin<30 мг/сутки (B)
- The combination of two Raas blockers is not recommended, despite the potential efficiency in reducing proteinuria (3a)
- Aldosterone antagonists cannot be recommended for SCF< 30 мл/мин/1,73м2, особенно в комбинации с блокатором РААС (3С)
- In case of insufficient effectiveness of funds blocking components of races, the antiproteinururic effect can be enhanced by adding NEDIHIDROPIRODINOVY BKK (2b)
- When applying the IAPF or sconium, and diuretics are recommended to control the level of creatinine and potassium serum (2C)
- It is recommended to constant control of the excretion of albumin with urine to assess the effectiveness of therapy and the rate of progression of the disease (2C)
Inhibitors of angiotensin gloculating enzyme and blockers to the at II receptor are recommended as drugs of the first series of choice for the treatment of diabetic nephropathy not only with an increase in blood pressure, but also when the appearance of Mau without arterial hypertension.
The feasibility of using Raas blockers is determined by the influence of angiotensin II - the consideration factor of the reduction of renal arteriole.
The clinically effect on the purpose of the RAAS blockers should be determined to reduce (previously elevated) blood pressure and reduce the excretion of protein with urine. The absence of such dynamics is not the reason for the abolition of the drug of this group, since even in this case its renoprotective action will be partially preserved.
Diuretics. The patient of the SD is not recommended to use thiazide diuretics in a dose of over 25 mg / day due to a dose-dependent diabetegenic effect. The mechanism of this effect is associated with a pronounced potassium-based action of these drugs, which leads to the loss of extracellular and intracellular potassium in the beta cells of the pancreas, followed by a violation of insulin secretion and the development of hyperglycemia. However, in a large-scale population study of Aric, which included more than 12,000 persons without SD, it was shown that the reception of thiazide diuretics at a dose of 12.5-25 mg per day for 6 years is not accompanied by an increase in the risk of development of SD 2.
Thiazid-like Diuretik Indapamide due to the minimum potassium effect does not have a diabetene effect and is safe in patients with high risk of development of the SD. The NESTOR study showed a comparable nephroprotective and cardioprotective effect of Indapamide Retard.
Tiazide diuretics / Indapamide in low doses are advisable to use at the SCF\u003e 50 ml / min, with lower values \u200b\u200bof the SCF, the use of loop diuretics (furosemid, thoramisident) is shown.
Calcium antagonists. Numerous clinical studies on the use of calcium antagonists (AK) in patients with ag confirmed the metabolic neutrality of these drugs. In the therapeutic doses, AK does not have a negative effect on carbohydrate and lipid metabolism, so it can be widely used in patients with diabetes for the treatment of AG.
Dihydropyridine AK as monotherapy is inappropriate to use as monotherapy due to their adverse effect on glomerular hemodynamics, but they can be used in combination with IAPF / sconce to enhance the antihypertensive effect.
In contrast, the antiproteinururic effect can be enhanced with the addition of non-nigidropyridine ACs with insufficient effectiveness of funds blocking components of the RAS (according to the results of large meta-analysis, which summarized numerous randomized proceedings on the use of ACs of this group, showing a decrease in the excretion of albumin with urine by an average of 30%).
Beta adrenoblocators. In patients with diabetes, as well as persons included in the high-risk group of SD 2 development (with obesity or metabolic syndrome), it is necessary to take into account the spectrum of metabolic side effects of Bab. Basically, all metabolic effects of women are associated with blockade of beta2-adrenoreceptors and are less pronounced in selective women. However, it is necessary to remember that the selectivity of women wears dose-dependent nature and disappears when the pre-dose of beta1-selective women is appointed.
With respect to the slowdown in the rate of decline of the SCF at DN, the reduction of albuminuria or proteinuria, almost all studies have noted the greater EAPF effectiveness compared to women. However, preparations of a group of women with vasodilatory activity - nonbivolol and carvedilol - can have an additional nephroprotective effect.
Glicosaminoglycans and proteinuria control
It is shown that, despite the multifactoric approach in the treatment of DN (rigid control of glycemia, maintaining the target level of blood pressure using the RAC blocking, the use of statins and aspirin), the development of albuminuria is prevented only in part of patients.
The use of a suloxide preparation containing a mixture of glycosaminoglycans, ensures the restoration of the charging systematic renal filter barrier and has a nephroprotective effect. Research di.n.a.s. It showed that the use of Sulodexide in a dose of 200 mg / day for 4 months leads to a decrease in the excretion of albumin with urine by more than 50% in 60% of patients with Mau.
In addition to the nephroprotective effect, the drug has an antithrombotic and anti-aggregation effect, improving hemodynamics in a microcirculatory line, and also contributes to a decrease in plasma lipids due to the activation of lipoprotein-lipase. According to the algorithms of specialized medical care for patients with diabetes of 2013 at the stages of Albuminuria A2 and A3, glycosaminoglycans (suloxide) can be used.
Recommendations for the treatment of dyslipidemia in patients with SD and HBS
- Limited hypolypidemic therapy with statins / ezetimib combination is shown to reduce the risk of cardiovascular events, including patients after kidney transplantation (1b)
- In patients, the purpose of hypolypidemic therapy is the level of LDL<2,5 ммоль/л и <1,8 ммоль/л для пациентов с сердечно-сосудистой патологией (2В)
- It is not recommended to begin hypolypidemic therapy in patients with SD on hemodialysis in the absence of specific cardiovascular testimony for their application (1b)
Patients with SD, HBP and Dlypidemia have the highest risk of developing cardiovascular pathology. Therefore, all international recommendations that determine the target values \u200b\u200bof the level of blood lipids at SD, first of all orient doctors to reduce cardiovascular risk.
Statins or their combination with esetimib is the treatment of choice, reducing oh, triglycerides and somewhat increasing HDL. At SPF<30 мл/мин дозировка аторвастатина и правастатина остается прежней, дозу других статинов необходимо снижать в 2-3 раза.
R.A. Nadeha, O.N. Sigitova
Diabetes in the modern world has long acquired unkind glory as noncommunicable epidemic.
The disease in recent years has grown substantially, among the patients of endocrinologists - and 30, and 20-year-olds.
If one of the complications - nephropathy may appear after 5-10 years, then when it is often stated at the time of diagnosis.
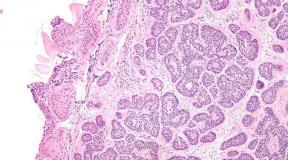
The diagnosis of diabetic nephropathy indicates a defeat in the kidney of filtering elements (glomers, tubular, arteries, arterioles) as a result of a failure in the metabolism of carbohydrates and lipids.
 The main reason for the development of nephropathy in diabetics is an increase in blood glucose.
The main reason for the development of nephropathy in diabetics is an increase in blood glucose.
At an early stage, the patient appears dryness, unpleasant taste in the mouth, general weakness and reduced appetite.
Also among the symptoms - increasing the amount of urine allocated, frequent night cues to urination.
About nephropathy There are also changes in clinical assays: a decrease in the level of hemoglobin, the specific weight of urine, an increased level of creatinine, etc. On more launched stages to the above symptoms added disorders in the work of the gastrointestinal tract, skin itching, swelling and hypertension.
Important!
If the patient is diagnosed with diabetes, it is necessary to take a blood test for creatin into creatin in a year once a year (with calculation speed of glomerular filtration) and a common urine analysis to control the state of the kidneys!
Differential diagnosis
In order to correctly determine the diagnosis, the doctor must make sure that the work of the kidneys gave the failure due to diabetes, and not other diseases.
The patient should be given a blood test for creatinine, urine on albumin, microalbumin and creatinine.
 The basic indicators for the diagnosis of diabetic nephropathy are albuminuria and the shorter filtration rate (hereinafter referred to as the SCF).
The basic indicators for the diagnosis of diabetic nephropathy are albuminuria and the shorter filtration rate (hereinafter referred to as the SCF).
At the same time, it is an increase in the excretion of albumin (protein) with urine indicative of the initial stage of the disease.
The SCF in the early stages can also give elevated values \u200b\u200bthat are reduced with the progression of the disease.
The SCF is calculated using formulas, sometimes through the trick of Rarba Tareev.
Normally, the SCF is equal to or more than 90 ml / min / 1.73m2. The diagnosis of "nephropathy of the kidneys" is a patient if he has a reduced level of SCF for 3 or more months and there is deviations in a general clinical analysis of urine.
4 main stages of the disease are distinguished:

Treatment
The main goals in the fight against nephropathy are inextricably linked with the treatment of diabetes as a whole. These include:
- reducing blood sugar levels;
- stabilization of blood pressure;
- normalization of cholesterol levels.
Medical drugs to combat nephropathy
 For the treatment of high pressure during diabetic nephropathy aCE inhibitors have proven well.
For the treatment of high pressure during diabetic nephropathy aCE inhibitors have proven well.
They generally affect the cardiovascular system well and reduce the risk of the last stage of nephropathy.
Sometimes the patients have a reaction in the form of dry cough on this group of drugs.Then, preference should be given to angiotensin-II receptor blockers. They are a bit more expensive, but do not have contraindications.
At the same time, apply APE inhibitors and angiotensin receptor blockers cannot be used.
With a decrease in the SCF patient, it is necessary to adjust the dose of insulin and sugar drugs. This can only do a doctor based on a common clinical picture.
Hemodialysis: Indications, Efficiency
Sometimes drug treatment does not give the desired results and the SCF becomes below 15 ml / min / m2, then the patient is prescribed renal renal therapy.
Also refer to its testimony:
- explicit increase in blood potassium level, which is not reduced by drugs;
- fluid delay in the body, which can cause severe consequences;
- visible symptoms of protein-energy failure.
One of the existing methods of substitution therapy, along with peritoneal dialysis and kidney transplantation, is hemodialysis.
To help the patient, it is connected to a special apparatus, which performs the function of artificial kidneys - purifies blood and the body as a whole.
 This treatment method is available in hospital departments, as the patient must be located near the device for about 4 hours 3 times a week.
This treatment method is available in hospital departments, as the patient must be located near the device for about 4 hours 3 times a week.
Hemodialysis allows you to profile blood, remove toxins from the body, poisons, normalize blood pressure.
Among possible complications are a decrease in blood pressure, infectious infection.
Contraindications for hemodialysis are: Heavy mental disorders, tuberculosis, cancer, heart failure, stroke, some blood diseases, age more than 80 years. But in very difficult cases, when a person's life rests on the hairs, there are no contraindications for hemodialysis.
Hemodialysis allows for a while to restore the kidney function, in general, he prolongs life for 10-12 years. Most often doctors use this treatment method as temporary before kidney transplantation.
Diet and prevention
Sick nephropathy is obliged to use all possible levers for treatment. The correctly chosen diet does not just help in this, but will improve the overall condition of the body.
 To do this, the patient follows:
To do this, the patient follows:
- minimally use protein food (especially animal origin);
- limit the use of salt during cooking;
- with a reduced level of potassium in the blood, add products rich in this element to the diet, rich in this element (bananas, buckwheat, cottage cheese, spinach, etc.);
- abandon sharp, smoked marinated, canned food;
- consulate high-quality drinking water;
- go to fractional food;
- limit in diet products with high cholesterol content;
- give preference to "right" carbohydrates.
 Low protein diet in food - Base for nephropathy patients. It has been scientifically proven that a large amount of protein food in the diet has a direct nephrotoxic effect.
Low protein diet in food - Base for nephropathy patients. It has been scientifically proven that a large amount of protein food in the diet has a direct nephrotoxic effect.
At different stages of the disease, the diet has its own characteristics. For microalbuminary protein in the general diet should be 12-15%, that is, no more than 1 g per 1 kg of body weight.
If the patient suffers with increased arterial pressure, you need to limit the daily use of salt up to 3-5 g (this is about one teaspoon). Food can not be acted daily calorieness not higher than 2500 calories.
At the stage of proteinuria protein use should be reduced to 0.7 g per kilogram of weight, and salts - up to 2-3 g per day. From the dietary patient must exclude all products with a high salt content, preference to give rice, oatmeal and semolina, cabbage, carrots, potatoes, some varieties of fish. Bread can only begged.
Diet at the stage of chronic renal failure involves a decrease in protein use to 0.3 g per day and limit in the diet of products with phosphorus. If the patient feels "protein starvation", it is prescribed drugs with indispensable essential amino acids.
In order for the low-tie diet to be effective (that is, he slowed down the progression of sclerotic processes in the kidneys) The doctor must achieve a rack compensation for carbohydrate metabolism and stabilize blood pressure in the patient.
The low-facility diet has not only advantages, but also its limitations and disadvantages. The patient must systematically monitor the level of albumin, trace elements, the absolute number of lymphocytes and erythrocytes in the blood. And also to keep a diary and regularly adjust your diet, depending on the above indicators.
- specific pathological changes in renal vessels arising from diabetes mellitus of both types and leading to glomerosclerosis, a decrease in the filtering function of the kidneys and the development of chronic renal failure (CPN). Diabetic nephropathy is clinically manifested by microalbuminuria and proteinuria, arterial hypertension, nephrotic syndrome, signs of Uremia and CPN. The diagnosis of diabetic nephropathy is based on the determination of the level of albumin in the urine, the clearance of endogenous creatinine, the protein and lipid spectrum of blood, the data of the ultrasound of the kidneys, the USDG of the renal vessels. In the treatment of diabetic nephropathy, diet, correction of carbohydrate, protein, fat metabolism, reception of ACE and ARA inhibitors, disintellation therapy, when necessary - hemodialysis, kidney transplantation is shown.

Diabetic nephropathy is a late complication of diabetes mellitus 1 and 2 types and one of the main causes of patients with this disease. Developing during diabetes damage to large and small blood vessels (diabetic macroengiath and microangiopathy) promote the damage to all organs and systems, first of all, the kidneys, eye, nervous system.
Diabetic nephropathy is observed in 10-20% of diabetic patients; Somewhat more often, nephropathy complicates the flow of an insulin-dependent type of disease. Diabetic nephropathy reveal more often in male patients and in persons with type 1 diabetes, developing in publity. The peak of the development of diabetic nephropathy (STNA stage) is observed with a duration of diabetes 15-20 years.
Causes of diabetic nephropathy
Diabetic nephropathy is due to pathological changes in the renal vessels and glomers of capillary loops (glomerulum) performing a filtration function. Despite the various theories of the pathogenesis of diabetic nephropathy, considered in endocrinology, the main factor and the launcher of its development is hyperglycemia. Diabetic nephropathy arises due to a long insufficient compensation of carbohydrate exchange disorders.
According to the metabolic theory of diabetic nephropathy, permanent hyperglycemia gradually leads to changes in biochemical processes: non-enzyme glycosylation of protein molecules of kidney glomers and a decrease in their functional activity; violation of water-electrolyte homeostasis, the exchange of fatty acids, a decrease in oxygen transport; Activation of the polyol route of glucose utilization and toxic effects on the kidney tissue, increasing the permeability of the renal vessels.
Hemodynamic theory In the development of diabetic nephropathy, the main role is assigned arterial hypertension and disorders of intravenous blood flow: the imbalance of the tone of bringing and increasing the arteriole and an increase in blood pressure inside the gloms. Long-term hypertension leads to structural changes of the gloms: first to hyperfiltration with the accelerated formation of primary urine and the yield of proteins, then to the substitution of the tissue tissue tissue on the connecting (glomerosclerosis) with the total occlusion of the glomerulos, a decrease in their filtration capacity and the development of chronic renal failure.
Genetic theory is based on a patient with diabetic nephropathy of genetically deterministic predisposing factors manifested in exchange and hemodynamic disorders. In the pathogenesis of diabetic nephropathy, all three development mechanisms are involved and closely interact.
The risk factors of diabetic nephropathy are arterial hypertension, long-term uncontrollable hyperglycemia, urinary tract infection, fatty metabolic infections and overweight, male floor, smoking, use of nephrotoxic drugs.
Symptoms of diabetic nephropathy
Diabetic nephropathy is a slowly progressive disease, its clinical picture depends on the stage of pathological changes. In the development of diabetic nephropathy, the stages of microalbuminuria, proteinuria and the terminal stage of chronic renal failure are distinguished.
For a long time, diabetic nephropathy proceeds asymptomatic, without any external manifestations. At the initial stage of diabetic nephropathy, an increase in the size of the kidney glomes (hyperfunctional hypertrophy), an increase in the renal blood flow and an increase in the flushing filtration rate (SCF) is noted. A few years later, the initial structural changes in the shortened kidney apparatus are observed from the debut of diabetes. The high volume of glomerular filtration is preserved, the excretion of albumin with urine does not exceed normal indicators (
Starting diabetic nephropathy develops more than 5 years from the beginning of pathology and manifests itself with permanent microalbuminuria (\u003e 30-300 mg / day or 20-200 mg / ml in the morning portion of urine). A periodic increase in blood pressure may be observed, especially during exercise. The deterioration of the well-being of patients with diabetic nephropathy is observed only in the late stages of the disease.
Clinically pronounced diabetic nephropathy develops after 15-20 years with type 1 diabetes mellitus and is characterized by a resistant proteinuria (protein level in the urine -\u003e 300 mg / day), indicating the irreversibility of the lesion. Renal blood flow and SCF decrease, arterial hypertension becomes constant and difficult to corrected. It develops nephrotic syndrome, manifested by hypoalbuminemia, hypercholesterolem, peripheral and strip swells. Creatinine and blood urea levels are normal or slightly elevated.
At the terminal stage of diabetic nephropathy, a sharp decrease in the filtration and concentration functions of the kidneys is noted: a massive proteinuria, a low SCF, a significant increase in the level of urea and creatinine in the blood, the development of anemia, expressed edema. At this stage, hyperglycemia, glucosuria, excretion with urine endogenous insulin, as well as the need for exogenous insulin can be significantly reduced. Progresses nephrotic syndrome, the blood pressure reaches high values, develops dyspepsive syndrome, Uremia and CPN with signs of the body's self-defense, the products of the exchange and damage of various organs and systems.
Diagnosis of diabetic nephropathy
The early diagnosis of diabetic nephropathy is an essential task. In order to establish a diagnosis of diabetic nephropathy, a biochemical and general blood test, biochemical and general analysis of urine, the trick of Rarga, the Zimnitsky sample, the USDG of the kidney vessels are carried out.
The main markers of the early stages of diabetic nephropathy are microalbuminuria and the speed of glomerular filtration. With the annual screening of patients with diabetes mellitus, investigate the daily excretion of albumin with urine or albumin / creatinine ratio in the morning portion.
The transition of diabetic nephropathy into the stage of proteinuria is determined by the presence of a protein in the overall analysis of urine or excretion of albumin with urine above 300 mg / day. There is an increase in blood pressure, signs of nephrotic syndrome. Late stage of diabetic nephropathy does not represent difficulties for diagnosis: to massive proteinuria and a decrease in the SCF (less than 30 - 15 ml / min), a rise of creatinine levels and blood levels (azotemia), anemia, acidosis, hypocalcemia, hyperliphosphamia, hyperlipidemia, swelling of the face And the whole body.
It is important to carry out the differential diagnosis of diabetic nephropathy with other kidney diseases: chronic pyelonephritis, tuberculosis, acute and chronic glomerulonephritis. For this purpose, a bacteriological study of urine on the microflora, ultrasound of the kidneys, an excretory urography can be performed. In some cases (with early developing and rapidly increasing proteinuria, the sudden development of nephrotic syndrome, rack hematuria) to clarify the diagnosis, a thin-game aspiration biopsy of the kidney is carried out.
Treatment of diabetic nephropathy
The main purpose of the treatment of diabetic nephropathy is to prevent and maximize further progression of the disease to CPN, reduce the risk of developing cardiovascular complications (IBS, myocardial infarction, stroke). Common in the treatment of different stages of diabetic nephropathy is strict control of blood sugar, blood pressure, compensation of disorders of mineral, carbohydrate, protein and lipid exchanges.
The preparations of the first choice in the treatment of diabetic nephropathy are inhibitors of an angiotensification enzyme (ACE): Enalapril, Ramipril, TranDolapril and receptor antagonists to angiotensule (ARA): Irbesartan, Valsartan, Lozartan, normalizing systemic and intraccurine hypertension and slowing the progression of the disease. Preparations are prescribed even with normal blood pressure in doses that do not lead to the development of hypotension.
Starting from the microalbuminuria stage, the low-tone, an abolishing diet is shown: restricting the consumption of animal protein, potassium, phosphorus and salt. To reduce the risk of developing cardiovascular diseases, the discharge of dyslipidemia is needed due to a diet with a low content of fat and drugs that normalize the lipid spectrum of blood (L-arginine, folic acid, statins).
At the terminal stage of diabetic nephropathy, disinfecting therapy is required, correction of diabetes treatment, the reception of sorbents, antioasemic agents, normalization of the hemoglobin level, the prevention of osteodistrophia. With a sharp deterioration of the kidney function, the question of conducting a patient of hemodialysis, permanent peritoneal dialysis or surgical treatment with a transplantation method of donor kidney is raised.
Forecast and prevention of diabetic nephropathy
Microalbuminuria with a timely appointed adequate treatment is the only reversible stage of diabetic nephropathy. At the stage of proteinuria, it is possible to prevent the progression of the disease to CPN, the achievement of the terminal stage of diabetic nephropathy leads to a state that is not compatible with life.
Currently, diabetic nephropathy and developing as a result of HPN are leading testimony to substitution therapy - hemodialysis or kidney transplantation. CPN due to diabetic nephropathy serves as a cause of 15% of all fatal outcomes among patients with type 1 diabetes younger than 50 years.
The prevention of diabetic nephropathy is the systematic observation of patients with diabetes mellitus in an endocrinologist-diabetologist, timely correction of therapy, permanent self-control of the level of glycemia, compliance with the recommendations of the attending physician.