Coxarthrosis (pediatrics). Conservative therapy or surgery: treatment of coxarthrosis of the hip joint Coxarthrosis ICD code 10 in adults
RCHR (Republican Center for Health Development of the Ministry of Health of the Republic of Kazakhstan)
Version: Clinical protocols of the Ministry of Health of the Republic of Kazakhstan - 2014
Coxarthrosis [arthrosis of the hip joint] (M16)
Pediatrics, Traumatology and pediatric orthopedics
general information
Short description
Expert advice
RSE at the RVC "Republican Center"
Healthcare Development"
Ministry of Health
And social development
Republic of Kazakhstan
Protocol No. 9
Coxarthrosis- this is deforming arthrosis of the hip joint, develops as a result of congenital and degenerative-dystrophic diseases of the hip joint. The degenerative process begins with articular cartilage. As a result, it becomes thinner and its shock-absorbing properties are lost.
Coxarthrosis can occur against the background of hip dysplasia or congenital hip dislocation, aseptic necrosis of the femoral head, Perthes disease, an inflammatory process, or as a result of trauma (bruise, dislocation, fracture, microtrauma). Coxarthrosis can be unilateral or bilateral.
I. INTRODUCTORY PART
Protocol name: Coxarthrosis
Protocol code:
ICD-10 code(s):
M16.0 Primary coxarthrosis bilateral
M16.1 Other primary coxarthrosis
M16.2 Coxarthrosis as a result of dysplasia, bilateral
M16.3 Other dysplastic coxarthrosis
M16.4 Post-traumatic coxarthrosis, bilateral
M16.5 Other post-traumatic coxarthrosis
M16.6 Other secondary coxarthrosis, bilateral
M16.7. Other secondary coxarthrosis
M16.9 Coxarthrosis, unspecified
Abbreviations used in the protocol:
HIV - human immunodeficiency virus
GP - general practitioner
ELISA - enzyme immunoassay
CT - computed tomography
Exercise therapy - therapeutic physical culture
CBC - complete blood count
BCC - circulating blood volume
ECG - electrocardiography
EchoCG - echocardiography
Date of protocol development: year 2014.
Protocol users: general practitioners, pediatricians, pediatric surgeons, pediatric traumatologists and orthopedists, medical rehabilitation specialists (physiotherapists, exercise therapy doctors).
Classification
Clinical classification
According to the degree of deformation of the femoral head:
1st degree: Characterized by periodic pain that occurs after physical activity (long walking or running). The pain is mainly concentrated in the area of the hip joint, less often it occurs in the area of the hip and knee joint. The pain usually goes away after rest. The range of movements is not limited, gait is not impaired, muscle strength is not changed. The x-ray shows minor bone growths, but they do not extend beyond the labrum. Bone growths are located around the inner or outer edge of the articular surface of the acetabulum. The neck and head of the femur are practically unchanged. The joint space is unevenly narrowed.
2nd degree: pain intensifies and is more intense, radiating to the groin area, thigh and occurring even at rest. Long walking causes lameness. Internal rotation and abduction of the hip are significantly limited. The radiograph shows bone growths both along the inner and outer edges of the acetabulum, extending beyond the boundaries of the cartilaginous lip. The head of the femur is deformed, increases in volume and has an uneven contour. In the most loaded parts of the head and acetabulum, cyst formation is possible. The neck of the femur widens and thickens. The gap of the hip joint narrows unevenly (to 1/3 - 1/4 of the initial height). Displacement of the head of the hip bone upward.
3rd degree: constant pain that occurs even at night. Movements in the joint are sharply limited, the muscles of the thigh, lower leg and buttocks atrophy. Due to the weakness of the hip abductor muscles, the pelvis tilts in the frontal plane, which leads to shortening of the limb on the affected side. When walking to reach the floor, the patient has to step on his toes and tilt his body to the painful side. This is how you have to compensate for the shortening of the limb and the tilt of the pelvis. The x-ray visualizes extensive bone growths on the side of the femoral head and the roof of the acetabulum. The joint space narrows sharply. The neck of the femur is significantly expanded.
Diagnostics
II. METHODS, APPROACHES AND PROCEDURES FOR DIAGNOSIS AND TREATMENT
List of basic and additional diagnostic measures
Basic (mandatory) diagnostic examinations performed on an outpatient basis:
X-ray of the hip joints in a direct projection.
Additional diagnostic examinations performed on an outpatient basis:
X-ray of the hip joints with functional tests;
CT scan of the hip joints to determine the degree of deformity;
The minimum list of examinations that must be carried out when referring for planned hospitalization:
Determination of blood group;
Determination of Rh factor;
General urine analysis;
HIV ELISA;
Markers for hepatitis (B, C) by ELISA;
Basic (mandatory) diagnostic examinations carried out at the hospital level:
Blood group determination
Determination of Rh factor;
Control radiograph of the hip joints.
Additional diagnostic examinations carried out at the hospital level:
General urine analysis;
Coagulogram (duration of bleeding and clotting time, prothrombin, fibrinogen, platelet adhesion and aggregation reaction, antithrombin);
Biochemical blood test (total protein, alanine aminotransferase, total cholesterol, bilirubin, direct bilirubin, creatinine, urea, glucose, potassium, sodium, phosphorus, calcium, chlorine);
CT scan of the hip joints;
Diagnostic measures carried out at the stage of emergency care: not carried out.
Diagnostic criteria
Complaints and anamnesis:
Complaints: for pain in the hip joint, lameness, increased fatigue.
Anamnesis: the disease manifests itself as a consequence of hip dysplasia, congenital hip dislocation, osteochondropathy of the femoral head.
With age, the above complaints increase.
Physical examination:
Detection of pain during physical activity;
Limitation of range of motion in the hip joint;
There is a chroma when walking;
Positive Trendelenburg sign.
Instrumental studies:
X-ray of the hip joint: narrowing of the joint spaces, bone growths along the edges of the articular cartilage (osteophytes), areas of ossification (ossification) of the articular cartilage, subchondral sclerosis - compaction of bone tissue under the cartilage, osteoporosis - rarefaction of bone tissue, torn fragments of synovial villi;
CT scan of the hip joint: narrowing of the joint spaces, bone growths along the edges of the articular cartilage, areas of ossification (ossification) of the articular cartilage, subchondral sclerosis - compaction of bone tissue under the cartilage, osteoporosis - thinning of bone tissue, detached fragments of synovial villi.
Indications for consultation with specialists:
Consultation with a pediatrician/GP (in case of concomitant somatic pathology);
Consultation with a surgeon (to exclude surgical pathology);
Consultation with a phthisiatrician (to exclude bone tuberculosis);
Consultation with an oncologist (in the presence of skeletal formations to exclude malignant formations);
Consultation with a cardiologist (for pain in the heart area and changes in ECG, EchoCG);
Consultation with a psychologist (if there are changes in psychological status);
Consultation with a geneticist (in the presence of hereditary aggravating factors and diseases);
Consultation with an endocrinologist (in case of concomitant endocrine pathology);
Consultation with an otorhinolaryngologist (to identify and treat chronic foci of infection);
Consultation with a dentist (to identify and treat chronic foci of infection);
Consultation with a medical rehabilitation specialist.
Differential diagnosis
Differential diagnosis
Table 1 Differential diagnosis of coxarthrosis
|
Sign |
Contractures | Coxarthrosis | Tuberculosis of the hip joint |
| Onset of the disease | As a consequence of trauma, a consequence of acute hematogenous osteomyelitis, and the result of surgical interventions on the joints | As a consequence of open and closed reduction of congenital and pathological hip dislocations | Typically, the primary tuberculosis focus is in the prebronchial glands or lungs, then it spreads hematogenously to the elements of the hip joint. |
| Chromata | Often | Not always | Often |
| Limitation of movements | Often | Often | Often |
| X-ray damage | Depending on the etiology of the disease, structural changes for each joint | The femoral head is structurally heterogeneous, reduced in height, and sclerotic changes are noted on the side of the roof of the acetabulum. | Depending on the stage of the disease, destructive polymorphic disorders of the femoral head and neck are noted |
| Mantoux test | negative | negative | negative |
Treatment abroad
Get treatment in Korea, Israel, Germany, USA
Get advice on medical tourism
Treatment
Treatment Goals :
Carrying out complex treatment aimed at eliminating pain, rehabilitating the patient in order to restore the functions of the hip joint;
Increased range of motion in the hip joint;
Elimination of contractures of the hip joint;
Surgical treatment aimed at “centring” (complete immersion) of the femoral head into the acetabulum, decompression of the hip joint and stimulation of the reparative process in the hip joint.
Treatment tactics
Non-drug treatment:
Diet: general table No. 15;
Mode: general.
Drug treatment
Antibacterial therapy:
in order to prevent postoperative complications:
. 1st generation cephalosporins: Cefazolin, 50-100 mg/kg, intravenously, once 30-60 minutes before surgery.
. 2nd and 3rd generation cephalosporins:
Cefuroxime, 50-100 mg/kg/day, in 3-4 administrations; intramuscularly or intravenously;
Or ceftriaxone, 20-75 mg/kg/day, in 1-2 injections, intramuscularly or intravenously;
Or cefaperazone, 50-100 mg/kg/day, in 2-3 injections, intramuscularly or intravenously;
. lincosamides:
Lincomycin
Intramuscularly, 10 mg/kg/day, every 12 hours,
Intravenous drip administration at a dose of 10-20 mg/kg/day, in one or more injections for severe infections and children aged 1 month and older;
.glycopeptides:
Vancomycin: 15 mg/kg/day, not more than 2 g/day, every 8 hours, intravenously, each dose should be administered over at least 60 minutes.
Pain therapy(in the postoperative period):
non-narcotic analgesics:
. paracetamol, 200 mg, tablets - at the rate of 60 mg per 1 kg of child’s body weight, 3-4 times a day. The interval between doses should be at least 4 hours. The maximum daily dose is 1.5 g - 2.0 g;
Paracetamol rectal suppositories 125, 250 mg - a single dose is 10-15 mg/kg of the child’s body weight, 2-3 times a day, every 4-6 hours;
Paracetamol suspension 120 mg/5 ml, for oral administration - a single dose of the drug is 10-15 mg/kg body weight, 4 times a day, the interval between each dose is at least 4 hours (dose for children aged 1 to 3 month is determined individually).
Paracetamol syrup for oral administration 2.4% 50 ml - children from 3 to 12 months, ½ -1 teaspoon (60 -120 mg); from 1 year to 6 years, 1-2 teaspoons (120-240 mg); from 6 years to 14 years, 2-3 teaspoons (240-360 mg), 2 - 3 times a day.
The maximum duration of treatment with paracetamol when used as an analgesic is no more than 3 days.
. ibuprofen suspension 100 mg/5ml - 200 ml, for oral administration, 7-10 mg/kg body weight, maximum daily dose - 30 mg/kg. The interval between doses of the drug should not be less than 6 hours. The duration of treatment is no more than 5 days, as an anesthetic.
opioid analgesics:
. tramadol 50 mg/ml -2 ml in solution for injection,
Children from 1 to 14 years: from 1 mg/kg to 2 mg/kg body weight intravenously, intramuscularly or subcutaneously. Intravenous injections should be given very slowly or they should be diluted in an infusion solution and given by infusion. The dose can be repeated at intervals of 4-6 hours.
. trimeperidine 2%-1 ml in solution for injection, children over 2 years old, dosage is 0.1 - 0.5 mg/kg body weight. Contraindicated for children under 2 years of age.
. morphine 2% 1 ml:
From 2 to 3 years, the single dose is 0.1 ml (1 mg of morphine), the daily dose is 0.2 ml (2 mg of morphine);
3-4 years: single dose - 0.15 ml (1.5 mg), daily dose - 0.3 ml (3 mg);
5-6 years: single dose - 0.25 ml (2.5 mg), daily dose - 0.75 ml (7.5 mg);
7-9 years: single dose - 0.3 ml (3 mg), daily dose - 1 ml (10 mg);
10-14 years: single dose 0.3-0.5 ml (3-5 mg), daily dose - 1-1.5 ml (10-15 mg).
Infusion therapy with crystalloid solutions for the purpose of replacing and correcting water-electrolyte metabolism:
. sodium chloride solution 0.9%- administer 20-30 ml/kg;
. dextrose 5%- on the first day, 6 g of glucose/kg/day is administered, subsequently - up to 15 g/kg/day.
Blood products for replacement purposes, depending on perioperative blood loss:
. fresh frozen plasma(with a deficit of circulating blood volume of more than 25-30%, caused by blood loss, with plasma INR of more than 1.5 (normal 0.7-1.0), intravenous transfusion at a dose of 10-20 ml/kg body weight);
. erythrocyte suspension(with a deficit of circulating blood volume of more than 25-30%, hematocrit less than 24%, a decrease in hemoglobin below 70-80 g/l due to blood loss, and the occurrence of circulatory disorders, a transfusion at a dose of 10-20 ml/kg body weight is indicated.
.platelet concentrate(if the platelet level decreases below 50*10/9, against the background of bleeding, with further maintenance of the platelet level 100*10/9 - intravenous transfusion of 1 dose per 10 kg of body weight).
Drug treatment provided on an outpatient basis: not provided.
Drug treatment provided at the inpatient level
List of essential medicines(having 100% probability of implementation):
Antibiotics:
Cefazolin 500 mg powder for solution for intravenous and intramuscular administration
Non-steroidal anti-inflammatory drugs:
Paracetamol, tablets 200 mg;
Paracetamol, rectal suppositories 125, 250 mg;
Paracetamol suspension for oral administration 120 mg/5 ml;
Paracetamol syrup for oral administration 2.4% 50 ml;
Ibuprofen, oral suspension 100 mg/5 ml - 200 ml bottle with dosing syringe.
Analgesics:
Tramadol - 50 mg/ml -1 ml solution for injection;
Trimepiridine - 1 or 2% - 1 ml solution for injection;
Morphine - 1% - 1 ml, solution for injection.
Plasma replacement and perfusion solutions:
Sodium chloride 0.9% - 500, 400, 200 ml solution for intravenous infusion (50%);
Dextrose 5% - 500, 400, 200 ml solution for intravenous infusion (50%);
List of additional medicines(less than 100% probability of completion)
Antibiotics:
Cefuroxime, powder for solution for injection and infusion 750 mg and 1.5 g;
Ceftriaxone, powder for solution for injection 0.5 g and 1.0 g;
Cefaperazone, powder for the preparation of a solution for intravenous and intramuscular administration 1.0 g;
Lincomycin, solution for intravenous and intramuscular administration, 300 mg/ml.;
Vancomycin, lyophilisate for solution for infusion, 500 mg, 1000 mg.
Drug treatment provided at the emergency stage: not provided.
Other treatments
Other types of treatment provided on an outpatient basis:
Physiotherapy;
Massage;
Orthotics.
Other types of services provided at the stationary level:
Dressings;
Cuff traction;
Physiotherapy
Massage;
Exercise equipment;
Orthotics.
Other types of treatment provided at the emergency stage: not provided.
Surgical intervention
Surgical intervention provided on an outpatient basis: not performed.
Surgical intervention provided in an inpatient setting
Methods of surgical treatment:
Tunnelization of the femoral neck and revascularization of the femoral neck and head;
Corrective osteotomies using extramedullary, intramedullary metal structures and transosseous osteosynthesis apparatus;
Hospitalization
Indications for hospitalization indicating the type of hospitalization
Indications for emergency hospitalization: not carried out.
Indications for planned hospitalization: presence of 2-3 degree coxarthrosis.
Information
Sources and literature
- Minutes of meetings of the Expert Council of the RCHR of the Ministry of Health of the Republic of Kazakhstan, 2014
- "Orthopedics - National Guide" S.P. Mironova, G.P. Kotelnikova - M.: GEOTAR 2008 1. Degenerative - dystrophic diseases of the hip joint (clinical and experimental study): monograph / E.A. Nazarov; State Budgetary Educational Institution of Higher Professional Education Ryaz State Medical University of the Ministry of Health of Russia. – Ryazan, 2013. 2. Divakov M.G. Aseptic necrosis of bones and justification of methods of their treatment (clinical and experimental study): abstract of thesis. .... Doctor of Medical Sciences / M.G. Divakov.-M., 1991. 3. Hori Y. Revitalization of the Ostreonecrotic Femoral Head by Vascular Bundle Transplantation / Y. Hori // Segmental Idiopathic Necrosis of the Femoral Head. – Berlin: Springer – Verlag. 1981. – P.47-54. 4. Agadzhanyan V.V. Musculoskeletal autoplasty in the treatment of aseptic necrosis of the femur / V.V. Agadzhanyan, A.D. Zamulin, G.F. Krasnikov //Orthopedics, traumatology and prosthetics. – 1988.-№10. – P.24-25. 5. Clinical recommendations for practitioners, based on evidence-based medicine. 2nd edition, GEOTAR, 2002.
Information
III. ORGANIZATIONAL ASPECTS OF PROTOCOL IMPLEMENTATION
List of protocol developers with qualification information:
1) Nagymanov Bolat Abykenovich, candidate of medical sciences, associate professor, JSC "National Scientific Center for Maternity and Childhood", head of the department of traumatology-orthopedics and vertebrology No. 1, chief freelance pediatric traumatologist-orthopedist of the Ministry of Health of the Republic of Kazakhstan;
2) Kharamov Isamdun Kaudunovich, candidate of medical sciences, head of the department of traumatology and orthopedics of the Republican Children's Clinical Hospital "Aksai" at the Republican State Enterprise at the RPV "Kazakh National Medical University named after S.D. Asfendiyarov;
3) Bektasov Zharylkasyn Kuanyshbekovich, head of the department of traumatology and orthopedics of the State Public Enterprise at the State Children's Hospital "City Children's Hospital No. 2" in Astana;
4) Drobysheva Lyudmila Vasilievna, doctor-rehabilitologist of the Republican Children's Clinical Hospital "Aksai" at the Republican State Enterprise at the RPE "Kazakh National Medical University named after S.D. Asfendiyarov";
5) Dyusembayeva Nazigul Kuandykovna, Associate Professor of the Department of General and Clinical Pharmacology of Astana Medical University JSC, therapist of the highest category, clinical pharmacologist.
Disclosure of no conflict of interest: are missing.
Reviewers:
Dzhenalaev Bulat Kanapyanovich, Doctor of Medical Sciences, Professor, Head of the Department of Pediatric Surgery, West Kazakhstan State Medical University named after M. Ospanov
Indication of the conditions for reviewing the protocol: Review of the protocol 3 years after its publication and from the date of its entry into force and/or in the presence of new methods and areas of treatment with a level of evidence.
Attached files
Attention!
- By self-medicating, you can cause irreparable harm to your health.
- The information posted on the MedElement website and in the mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Guide" cannot and should not replace a face-to-face consultation with a doctor. Be sure to contact a medical facility if you have any illnesses or symptoms that concern you.
- The choice of medications and their dosage must be discussed with a specialist. Only a doctor can prescribe the right medicine and its dosage, taking into account the disease and condition of the patient’s body.
- The MedElement website and mobile applications "MedElement", "Lekar Pro", "Dariger Pro", "Diseases: Therapist's Directory" are exclusively information and reference resources. The information posted on this site should not be used to unauthorizedly change doctor's orders.
- The editors of MedElement are not responsible for any personal injury or property damage resulting from the use of this site.
Exercise therapy.
It must be remembered that weight loss measures must be combined with exercise therapy. Physical methods play an important role in the treatment of the disease, as they help improve joint function and increase endurance and muscle strength. Regular exercise therapy classes lead to a reduction in pain and improvement in joint movements, but it is best to start classes under the guidance of a specialist in physical therapy, for example, in health groups. Physical exercises should be carried out without static loads (sitting, lying down, in the pool). Patients with severe joint pain and contractures need to consult a physical therapy specialist to create an individual exercise program. The main principle of exercise therapy is frequent repetition of exercises throughout the day. You should not do exercises while overcoming pain. Perform the exercises slowly, smoothly, gradually increasing the load. You need to exercise for at least 30–40 minutes a day, 10–15 minutes several times during the day. For osteoarthritis of the knee joints, the main ones are exercises that help strengthen the thigh muscles (for example, raise a straight leg by 25 cm while lying on your back and hold it for several seconds); exercises aimed at increasing range of motion (“air bike”); exercises that help improve the general aerobic condition of the muscles (walking on level ground at a moderate pace).Treatment consists of a comprehensive approach to the disease, which involves the use of non-drug and medicinal methods, and, if necessary, surgical intervention. Although osteoarthritis is a chronic disease, treatment interventions tailored to each patient can reduce pain and inflammation, improve joint movement, and slow progression. It is important that the diagnosis be made by a doctor, since there are a number of other joint diseases that have similar symptoms to osteoarthritis.
As for drug therapy, it is stage-by-stage and individually selected by a specialist. Do not self-medicate and seek help. The more correct and timely the treatment is prescribed, the greater the chance of regaining the lost quality of life.
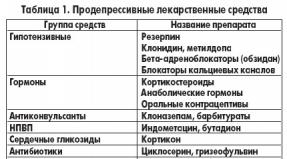
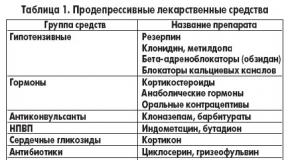
Orthopedists treat coxarthrosis. The choice of treatment methods depends on the symptoms and stage of the disease. At stages 1 and 2 of coxarthrosis, conservative therapy is carried out. During the period of exacerbation of coxarthrosis, non-steroidal anti-inflammatory drugs (piroxicam, indomethacin, diclofenac, ibuprofen) are used. It should be borne in mind that drugs in this group are not recommended to be taken for a long time, since they can have a negative effect on internal organs and suppress the ability of hyaline cartilage to recover.
To restore damaged cartilage due to coxarthrosis, agents from the group of chondroprotectors (chondroitin sulfate, calf cartilage extract, etc.) are used. To improve blood circulation and eliminate spasm of small vessels, vasodilators (cinnarizine, nicotinic acid, pentoxifylline, xanthinol nicotinate) are prescribed. Muscle relaxants (medicines to relax muscles) are used according to indications.
For persistent pain syndrome, patients suffering from coxarthrosis may be prescribed intra-articular injections using hormonal drugs (hydrocortisone, triamcinolone, metipred). Treatment with steroids must be done with caution. In addition, for coxarthrosis, local remedies are used - warming ointments, which do not have a pronounced therapeutic effect, however, in some cases they relieve muscle spasms and reduce pain due to their “distracting” effect. Also, for coxarthrosis, physiotherapeutic procedures are prescribed (phototherapy, ultrasound therapy, laser therapy, UHF, inductothermy, magnetic therapy), massage, manual therapy and therapeutic exercises.
A diet for coxarthrosis does not have an independent therapeutic effect and is used only as a means of weight loss. Reducing body weight allows you to reduce the load on the hip joints and, as a result, alleviate the course of coxarthrosis. In order to reduce the load on the joint, the doctor, depending on the degree of coxarthrosis, may recommend that the patient walk with a cane or crutches.
In the later stages (with coxarthrosis of the 3rd degree), the only effective method of treatment is surgery - replacing the destroyed joint with an endoprosthesis. Depending on the nature of the lesion, either a unipolar (replacing only the femoral head) or a bipolar (replacing both the femoral head and acetabulum) prosthesis can be used.
Endoprosthesis replacement surgery for coxarthrosis is carried out as planned, after a full examination, under general anesthesia. In the postoperative period, antibiotic therapy is carried out. The sutures are removed on days 10-12, after which the patient is discharged for outpatient treatment. After endoprosthetics, rehabilitation measures are required.
In 95% of cases, joint replacement surgery for coxarthrosis ensures complete restoration of limb function. Patients can work, move actively and even play sports. The average service life of a prosthesis, if all recommendations are followed, is 15-20 years. After this, a repeat operation is necessary to replace the worn endoprosthesis.
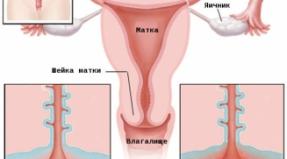
Dysplastic coxarthrosis is a disease whose appearance is caused by congenital pathology of underdevelopment of the hip joint. The disease is characterized by degenerative-dystrophic changes in the bony ends of the joint with the formation of a new shape of the latter and the depth of the acetabulum. In other words, this is arthrosis of the hip joint.
Etiology of disease formation
In the international classification, the disease of dysplastic coxarthrosis is assigned the code M16.2, M16.3. About half of all identified cases are the result of residual defects in joint development in children due to surgical or conservative treatment.
The development of the disease is facilitated by any pathology in the development of the pelvic bones or lower extremities in a child.
Dysplastic arthrosis is characterized by progressive development and manifestation in the early stages. It is important to carry out treatment promptly and promptly, since the disease leads to loss of ability to work, disability and significantly worsens the patient’s quality of life.
According to statistics, women are more likely to suffer from this pathology (about 80% of all diagnosed cases). Damage to the right hip occurs 3 times less frequently; bilateral lesions account for a quarter of all cases. Coxarthrosis is based on improper formation of articular tissues.
Due to difficulties in treatment, the patient often needs to have a prosthesis installed to maintain mobility of the hip joint. The congenitality of the pathology is due to the development of dysplasia, which is facilitated by the breech presentation of the fetus, its gender (female), hereditary factor, race and status of the first-born.
Changes in the joint

Degrees, forms and stages of the disease
Varieties of forms of the disease are determined by the localization of the central site of inflammation. Thus, dysplastic coxarthrosis can affect:
- Upper articular part. caused by the action of large loads on the joint.
- Central articular part. Pathological manifestations of this form have the most pronounced symptoms.
- The lower articular part. The most secretive type of disease, which has no obvious signs.
Until the age of 25, the process of renewal of cartilage tissue and the process of their breakdown are in balance. After this point, it changes due to a slowdown in synthesis. Cartilage wears out faster than it can regenerate. Depending on the duration of action of the factors predisposing its destruction, the process goes through 3 main stages, each of which has its own clinical picture.
The marginal growth of coarse scar tissue of cartilage occurs against the background of excessive load and injury. under pressure, but at rest there is no sound. This development of the disease is typical for the first stage.
Reactive tissue proliferation leads to a repeated inflammatory process. It, in turn, is accompanied by pain when moving not only in the joint area, but also along the entire front part of the thigh.
At the last stage, the pain does not stop even at rest, the person is not able to independently take care of himself in everyday matters. Posture and gait change.
 Despite its progressive development, dysplastic coxarthrosis does not always have obvious signs. The clinical picture of an active inflammatory process of the hip joints is characterized by:
Despite its progressive development, dysplastic coxarthrosis does not always have obvious signs. The clinical picture of an active inflammatory process of the hip joints is characterized by:
- The appearance of periodic or
- Stiffness of the affected joint
- Stiffness in movement
- Change in gait
- Muscle atrophy
- Lameness
The pain that arises can “walk” not only in the hips and groin area, but also down to the knees. With severe muscle atrophy, the buttocks and legs of the lower extremities are involved in the pathological process. deviation from the axis of the pelvic bones causes shortening of one of the legs.
Principles of arthrosis treatment

Treatment of dysplastic coxarthrosis
To make a diagnosis, a visual examination by a specialist is sufficient. allows you to clarify the stage and extent of joint damage.
The image will clearly show growths on the bones, the size of the joint space, the displacement of the bone head and its expansion. An orthopedist and a surgeon provide treatment and consultation to the patient.
Conservative therapy for dysplastic coxarthrosis is ineffective. Taking medications can only slightly slow down the process of tissue destruction. An integrated approach is required, including:
- Physical therapy
- Diet
- Endoprosthetics
The main group of prescribed drugs are. They are used in the form of ointments, gels, tablets or capsules. It may be necessary to introduce hormonal agents into the joint cavity. Severe muscle spasm and... Gymnastic exercises help prevent complete immobilization of the joint.
If there is no positive effect from the course, surgery is performed. There are several types of intervention: arthroplasty, joint suspension, osteotomy, prosthetics.
At the last stage of the disease, when the hip joint is destroyed, it is completely removed and a prosthesis is installed. The operation is effective, but expensive. But it allows the patient to maintain his ability to work and avoid disability.
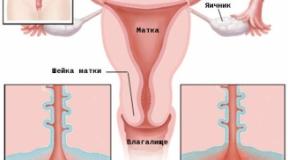
The photo shows dysplastic arthrosis of the hip joint

In medical practice, a special international classification of diseases (ICD-10) is used. But few people know what this code is and what number it contains post-traumatic coxarthrosis. The ICD-10 code is a good way to classify a disease and make an accurate clinical diagnosis.
System Description
The International Classification of Diseases, 10th revision, contains a list of common diseases that are welcomed in different countries of the world that are part of the global medical community. The system is intended to indicate the level of development of healthcare, as well as to establish medical standards for pathologies.
Using this code, doctors divide diseases into separate groups, identifying them by class, type, nature of course, and stage of development. In this way, they create an accurate clinical picture that will be understandable to doctors around the world. That is, this significantly simplifies consultations with specialists from other parts of the world and allows you to find joint methods for more productive treatment. Once every ten years, changes are made to the ICD, which are approved by the World Health Organization.
Currently, the current edition is ICD-10, i.e. the classification of the tenth revision. It contains all the pathologies known to modern medicine, which simplifies communications with international specialists, and also allows you to think through joint courses of therapy.
The system is especially important in emergency situations when it is necessary to transport a patient to another country for urgent treatment. Pathologies in ICD-10 are designated by a specific alphanumeric code and are found in one of 22 categories. The international classification combines existing diseases into a convenient system and also separates treatment methods. In this regard, it can be called a key document of contemporary medicine.
Purpose of classification
As already mentioned, the international classification of diseases covers many countries of the world that are members of the global association of health authorities, therefore the established system significantly simplifies the interaction of specialists from different countries of the world. When conducting a diagnosis, the attending physician draws up an accurate clinical picture and designates it with the appropriate code registered in ICD-10.
Knowing this code, the patient can provide doctors in any country with his diagnosis without any difficulties or explanations, and also receive an answer to his question. This practice is incredibly convenient, because it is much easier to point to an alphanumeric code than to remember a complex official diagnosis with many incomprehensible symbols.

Post-traumatic coxarthrosis
One of the most common joint diseases, which has its own designation in the international system, is post-traumatic coxarthrosis. ICD-10 classifies it as M15-M19.
The pathology is characterized by the onset of dystrophic-degenerative changes that disrupt the normal functionality of large joints of the human body. The progression of the disease causes destruction of the interarticular cartilage, which leads to discomfort due to chafing of the cartilage tissue. The lack of effective treatment threatens with dangerous complications, including the need for disability.
As you know, the upper part of the bone is covered with cartilage, which can compress under any load and secrete a special synovial fluid. Its task is to lubricate the moving elements of the joint. At rest, the cartilaginous structure expands, and when moving it acts as a shock absorber.
With the development of coxarthrosis, the natural lubricant becomes very thick and is no longer able to cope with its task. As a result, the cartilage begins to dry out and become deformed, and the bones come into contact with each other and are destroyed due to intense friction.
Primary coxarthrosis can be either left- or right-sided. Often it has an unknown etiology and does not have severe symptoms. The development of secondary coxartosis occurs against the background of cancer, trauma and inflammatory processes in the hip joint. Necrosis of the femoral head also contributes to this.
Unfortunately, pathological changes are irreversible, but if you take the necessary measures in time, diagnose and begin treatment, this will prevent the last stage of the disease and avoid complete destruction of the joints. If therapy is delayed, coxarthrosis will quickly move from one stage to the next. In this regard, the risk of patient disability will increase due to decreased ability to work or limited mobility.
Predisposing factors
There is an opinion that post-traumatic coxarthrosis of the hip joint or any other anatomical area occurs against the background of age-related changes. The fact is that, according to statistics, after 40 years such a pathology manifests itself in every tenth patient, and after sixty - in every third. As for people over 70 years of age, the problem is diagnosed in 80% of cases.
However, no one is immune from dystrophic-degenerative disorders, so they develop at a young age. This may be accompanied by the following predisposing factors:

- Genetic predisposition to joint disorders or developmental disorders of the joints. The problem may not make itself felt for a long time, but as you grow older or with intense exercise, symptoms will periodically appear.
- Damage to joints due to increased stress. This phenomenon often occurs in professional athletes or in overweight people. Also, the occurrence of coxarthrosis is accompanied by injuries and infections that affect musculoskeletal functions.
- A number of diseases of the musculoskeletal system that cause pathological redistribution of loads.
- Failures in the cardiovascular system and impaired blood circulation.
Experts say that the cause of coxartosis is a combination of predisposing factors, and if the patient has a predisposition to such a pathology, then it will begin to manifest itself much earlier. Patients with diabetes, excess weight and other abnormalities are at increased risk.
Symptoms and signs

Symptoms and signs
In the early stages, coxarthrosis can occur without pronounced symptoms. They appear only after intense exercise, localizing in the groin area, thigh and knee joint.
In most cases, the primary forms of pathology affect the knee area, so many patients come to the clinic with a desire to clarify the cause of discomfort in this place. An inexperienced rheumatologist may prescribe an x-ray examination, which will result in a false diagnosis of grade 1 gonarthrosis. In order not to waste time on unsuccessful treatment for another disease, you need to immediately undergo a comprehensive diagnosis and consult with a trained specialist.
If treatment for post-traumatic arthrosis of the hip joint is not started, other symptoms may be added to the pain. Among them:
- Severe stiffness of movement.
- Changed gait.

- Severe stiffness of movement.
- Crunching noise when performing daily activities.
- Changed gait.
As the disease progresses, exacerbations and remissions are noticed. This causes swelling of the joints, as well as the formation of chronic reflex spasms. The patient may experience discomfort when moving, muscle cramps, and fever. Over time, the joint begins to change shape, which can be seen upon visual inspection. In chronic stages, it becomes completely curved.
Stages of development
To conveniently diagnose the disease and then classify it according to the ICD code, doctors distinguish three stages of development of coxarthrosis. They are characterized by special symptoms and the nature of their course. The differences between different forms of pathology are as follows:

- The first stage is the least noticeable in terms of symptoms, since during it degenerative changes only begin. The first signs in the form of pain may appear due to intense exercise, professional sports, as well as a long stay at rest. The pain remains moderate, and there is no stiffness in movements yet. On an x-ray, you can notice a slight narrowing of the joint space, as well as rare bone outgrowths. If you start effective treatment, you can get rid of the problem in a short time, preventing its further development.
- With the second degree of coxarthrosis, aching pain develops, which is felt even during rest. Any movement of the legs becomes very difficult, it is difficult for the patient to lift or move the limbs to the side, and when turning the foot, the pain syndrome becomes unbearable. When walking, a crunching sound is heard in the joints, and lameness also appears. During the examination, using X-rays, it is possible to determine the deformation of the femoral head, all kinds of osteophytes and narrowing of the joint gap. Radical treatment methods can delay complications for several years.
- The latest degree of coxarthrosis is the third - chronic. During this period, the patient is bothered by unbearable, persistent pain that practically does not subside, muscle joints begin to atrophy, and inflammatory processes begin throughout the body. The x-ray image clearly shows deformation changes and narrowing of the joint space. Conservative treatment methods for the third stage are practically useless, and the only solution is surgical intervention, namely the arthroplasty method.
To make an adequate diagnosis of the pathology, the specialist will also use an external examination, carefully studying the moving functions of the leg, and the results of the x-ray. If there are any doubts about the correctness of the clinical picture, the patient is re-sent to MRI or CT.

Methods of diagnosis and treatment
To make a diagnosis of post-traumatic arthrosis, it is necessary to take into account the medical history, clinical manifestations and X-ray results. They clearly show any deviations from the norm, including deformation of the articular area, the development of osteophytes, osteosclerosis and strange neoplasms. If the disease has entered a chronic stage, causing subluxation, this will disrupt the axis of the limb and lead to unevenness of the joint space.
If a more in-depth diagnosis is necessary, the patient is prescribed a computed tomography scan, and an MRI of the joint is used to determine pathological changes. In particularly difficult cases, the option of using arthroscopy is considered - a special technique that analyzes the condition of cartilage tissue, ligaments and other joints. The procedure is relevant when diagnosing the knee.
As for the methods of treating pathology, there are a lot of them. But before choosing a suitable technique, you need to consult with a professional orthopedist or traumatologist to draw up a clinical picture and prepare a course of therapy.
Regardless of the method used, it should be aimed at eliminating or reducing pain, restoring joint mobility, and preventing its destruction in the future. It is important to carry out complex therapy, which consists of taking non-steroidal anti-inflammatory drugs, chondroprotectors, gymnastics, massage and thermal procedures, laser therapy, etc.
Surgical intervention is prescribed in particularly difficult cases when conservative methods are useless. Surgery can restore the configuration and stability of joints when they are in a chronic condition. If the articular surfaces are severely deformed, they are replaced with an endoprosthesis. Also, during surgical intervention, various metal structures are introduced into the joints, which promote the regeneration of the joints.
The effectiveness of surgery is determined by many factors. First of all, the stage and nature of the pathology, as well as the specificity of the symptoms, are taken into account. In advanced forms of arthrosis, complete restoration of the joint is impossible. In this case, the only way out of the situation is to install a prosthesis.
Conservative approach

Conservative approach
When fighting arthrosis, a variety of techniques are used. This may include medications, as well as physical therapy exercises. To prevent surgical intervention and reduce financial costs, you need to undergo a full course of conservative therapy, which includes taking painkillers and anti-inflammatory medications, various exercises, massage treatments, hirudotherapy and other solutions.
In addition to tablets and ointments, the patient is prescribed physiotherapeutic procedures and kinesitherapy. He also needs to reconsider his diet, giving up fatty and unhealthy foods. The right approach and caring attitude towards your health is the key path to successfully eliminating the manifestations of coxarthrosis.